71 yo CM is admitted to the hospital with CC: SOB for 3 weeks. The patient is on home O2 and CPAP and despite using aerosols and his CPAP machine, SOB is getting worse. One week prior to admission he found that his oxygen machine was not working. The patient had also noticed that his hands and feet were getting bluish in color for the past two weeks. He was at his physician's office where he was found to have SpO2 of 70% and hence was advised to be admitted for further management. The patient denied fever, chills and cough. No history of CP or palpitations.
PMH: HTN, DM 2, COPD. Atrial fibrillation, OSA on CPAP 13 cm H2O and 5 L oxygen, pulmonary hypertension, CHF, CRI, Obesity
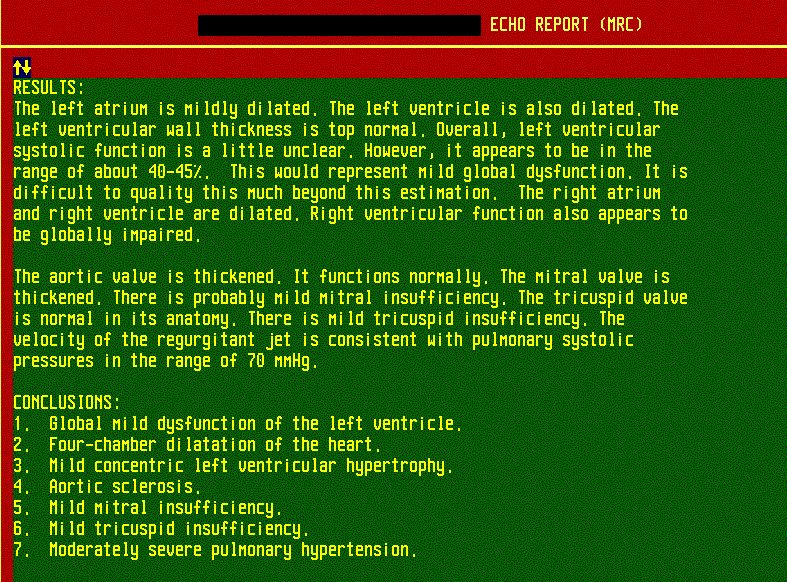
The patient had a sleep study one year ago which confirmed severe OSA. He had a 2-D echo at the same time which revealed moderate to severe pulmonary hypertension (70 mmHg), EF 40% to 45%.

2D Echo showed pulmonary hypertension with a PA pressure of 70 mm Hg
Medications: Actos, Amaryl, verapamil, Lasix, Coumadin, Flonase
SH: 50-pack-year history of smoking. He quit four years ago. He denies drinking alcohol or using illicit drugs.
Physical examination:
Obese man, dyspneic at rest.
VS 36.4-108-20-109/72
SpO2 85% to 88% on 5 L nasal cannula
Lungs: Decreased air entry bilaterally. No wheeze or crackles
CVS: Irregular rhythm
Abdomen: obese, protuberant
Extremities: 2+ pedal edema with bilateral chronic stasis changes. Skin of the fingers and toes is cyanotic and cold.




Acrocyanosis in a patient with polycythemia and hypoxemia

Cyanosis of the lips and tongue
EKG revealed atrial fibrillation, rate controlled, a low amplitude base and no acute ischemic changes.

CBD shows polycythemia due to persistent hypoxemia

CXR report

ABGs in Pickwickian syndrome
What happened?
He was started on CPAP with a pressure of 13 cm of water with oxygen titrated for a pulse oximetry of more than 94%.
The patient was also started on IV steroids and IV Lasix. He was advised to be on oxygen throughout the day with CPAP at night. The cyanosis in the extremities gradually resolved.
He was discharged to a transitional care unit.
Final diagnosis: End-stage respiratory failure. Cor pulmonale due to COPD, Pickwickian syndrome, OSA.
PMH: HTN, DM 2, COPD. Atrial fibrillation, OSA on CPAP 13 cm H2O and 5 L oxygen, pulmonary hypertension, CHF, CRI, Obesity
The patient had a sleep study one year ago which confirmed severe OSA. He had a 2-D echo at the same time which revealed moderate to severe pulmonary hypertension (70 mmHg), EF 40% to 45%.
2D Echo showed pulmonary hypertension with a PA pressure of 70 mm Hg
Medications: Actos, Amaryl, verapamil, Lasix, Coumadin, Flonase
SH: 50-pack-year history of smoking. He quit four years ago. He denies drinking alcohol or using illicit drugs.
Physical examination:
Obese man, dyspneic at rest.
VS 36.4-108-20-109/72
SpO2 85% to 88% on 5 L nasal cannula
Lungs: Decreased air entry bilaterally. No wheeze or crackles
CVS: Irregular rhythm
Abdomen: obese, protuberant
Extremities: 2+ pedal edema with bilateral chronic stasis changes. Skin of the fingers and toes is cyanotic and cold.




Acrocyanosis in a patient with polycythemia and hypoxemia

Cyanosis of the lips and tongue
EKG revealed atrial fibrillation, rate controlled, a low amplitude base and no acute ischemic changes.
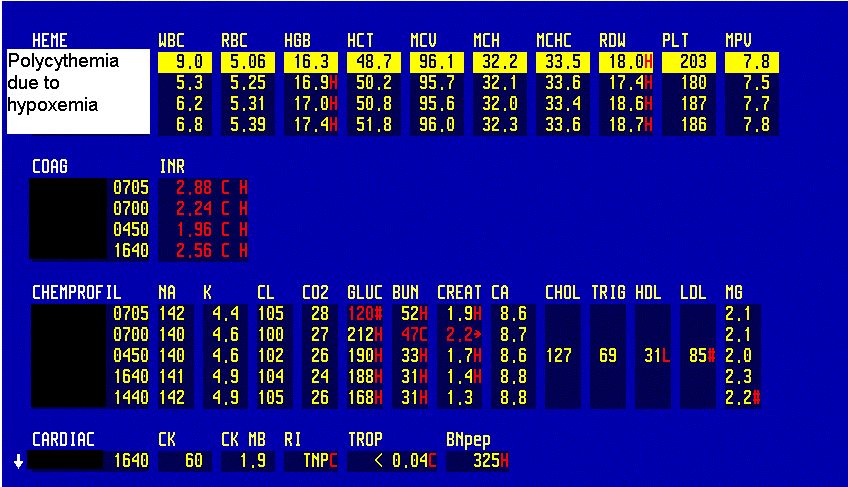
CBD shows polycythemia due to persistent hypoxemia

CXR report
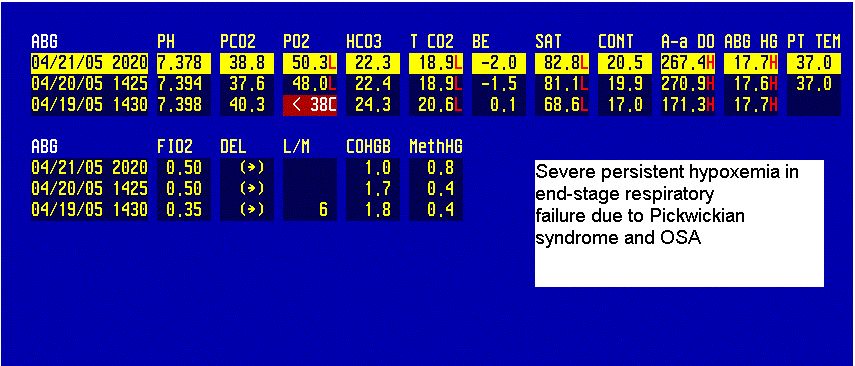
ABGs in Pickwickian syndrome
What happened?
He was started on CPAP with a pressure of 13 cm of water with oxygen titrated for a pulse oximetry of more than 94%.
The patient was also started on IV steroids and IV Lasix. He was advised to be on oxygen throughout the day with CPAP at night. The cyanosis in the extremities gradually resolved.
He was discharged to a transitional care unit.
Final diagnosis: End-stage respiratory failure. Cor pulmonale due to COPD, Pickwickian syndrome, OSA.