56 yo AAM was seen in the ER for bronchitis one year ago. The CXR showed a RUL mass and the patient was told to follow-up with his physician but he never did.
Now, he complains of cough productive of yellow sputum for about one week, and reports some weight loss but he cannot say how much.
PMH: Smoker, EtOH abuse
Medications: none
SH: Smoker - 30 pck-yr, quit 2 weeks ago, drinks 1 pint of liquor per day
Physical examination: Thin man in NAD
VS 37.7-105-137/61-18.
Chest: breath sounds are reduced in the right upper lobe
CVS: Clear S1S2
Abdomen: Soft, NT, ND
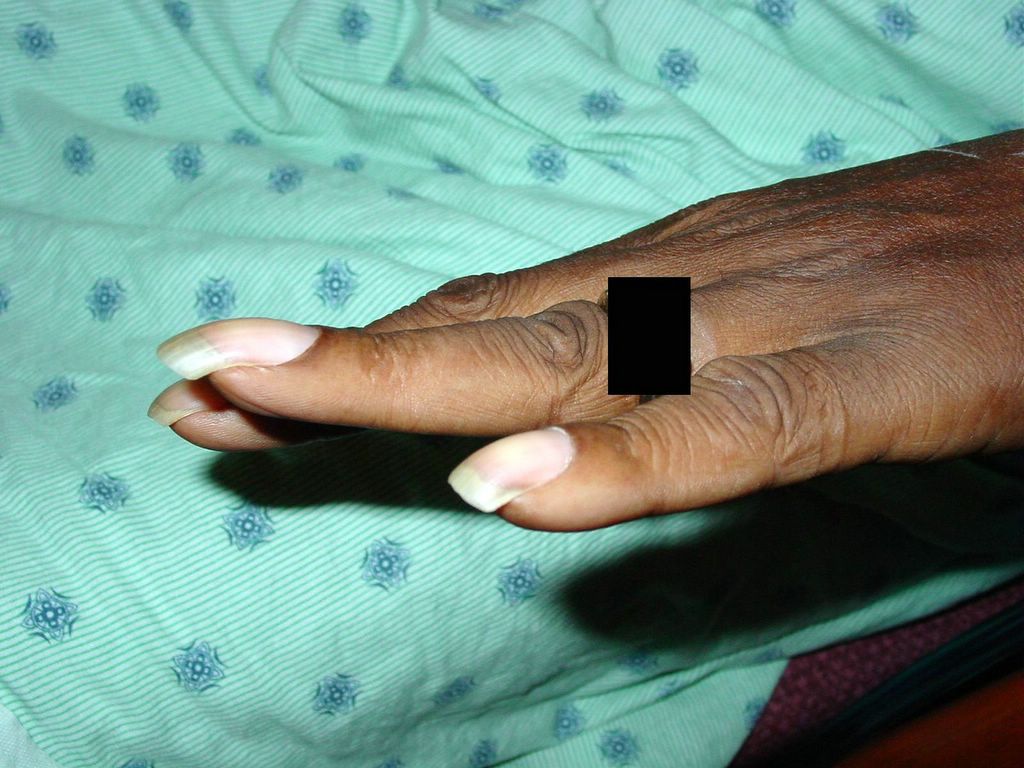
Extremities: clubbing



Clubbing in a long-term smoker with suspected lung cancer
What do you think is going on?
Pneumonia?
TB?
Cancer?
What tests would you order?
CXR
CBCD, CMP

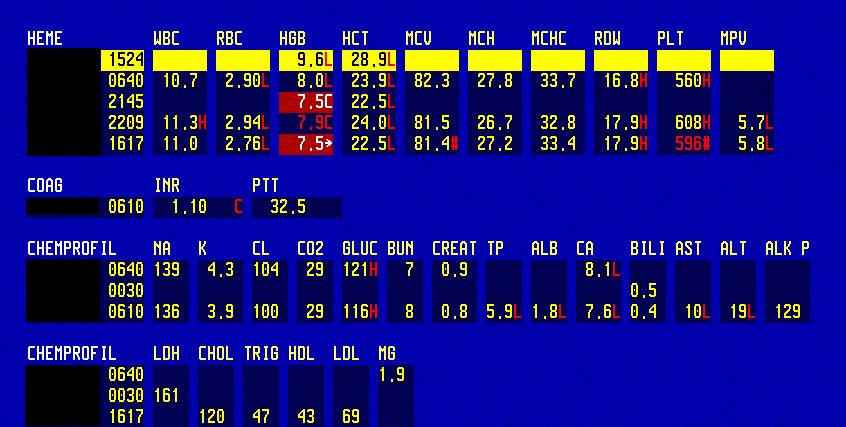
CBC shows anemia due to iron deficiency, malnutriton (note Alb level is 1.8), alcohol abuse and chronic disease
CXR



PA CXR showed a small RUL mass one year ago. The patient was advised to follow-up with his physician and to have a CT scan of the chest but he was drinking heavily at the time and he never followed up on the findings. Close-up of the RUL mass. Previous CXR report.



The RUL mass seen on the previous CXR one ago, has strikingly increased in size. Lateral film shows a large RUL mass. CXR report.
CT of the chest

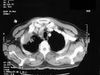
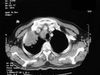


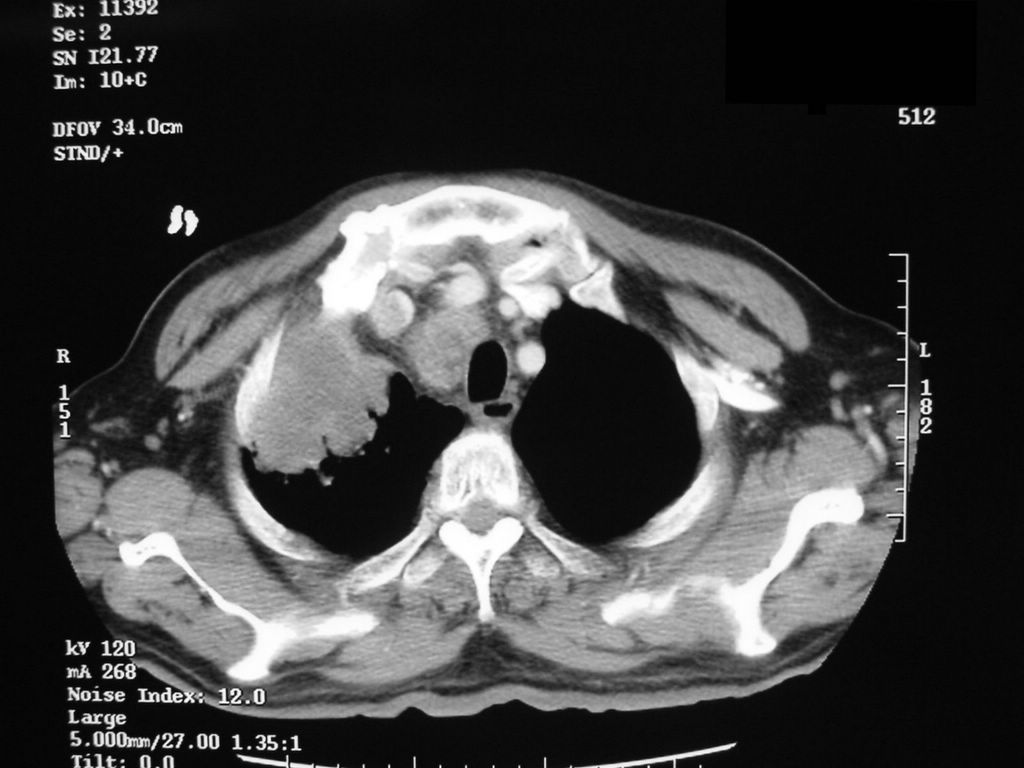
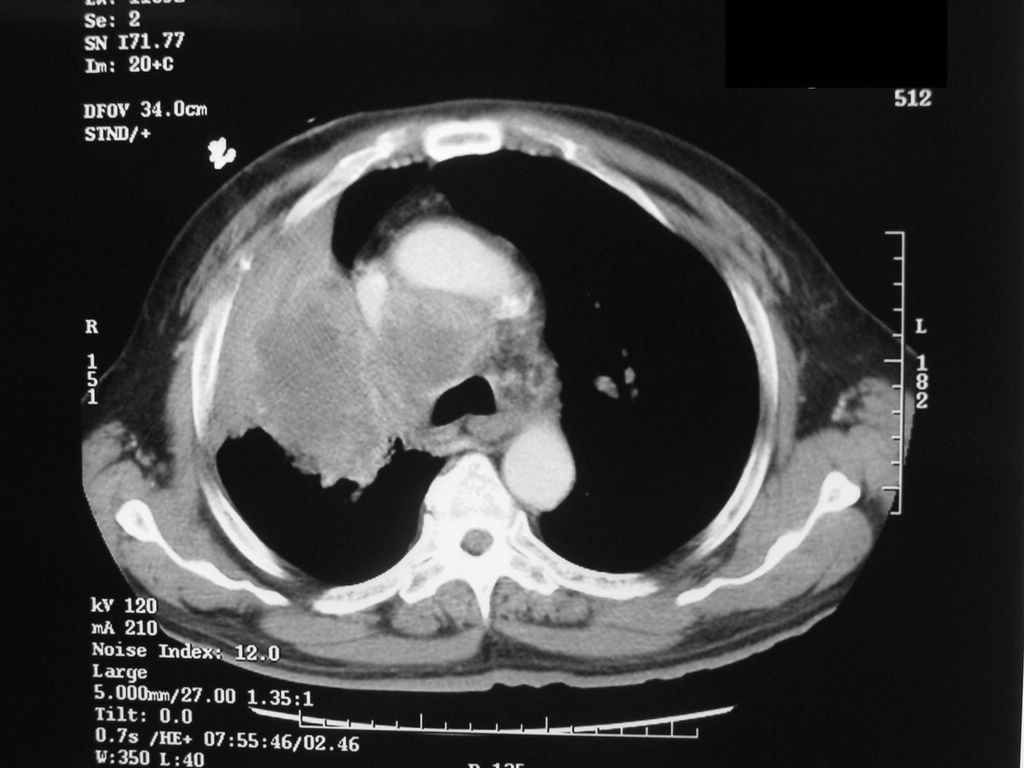
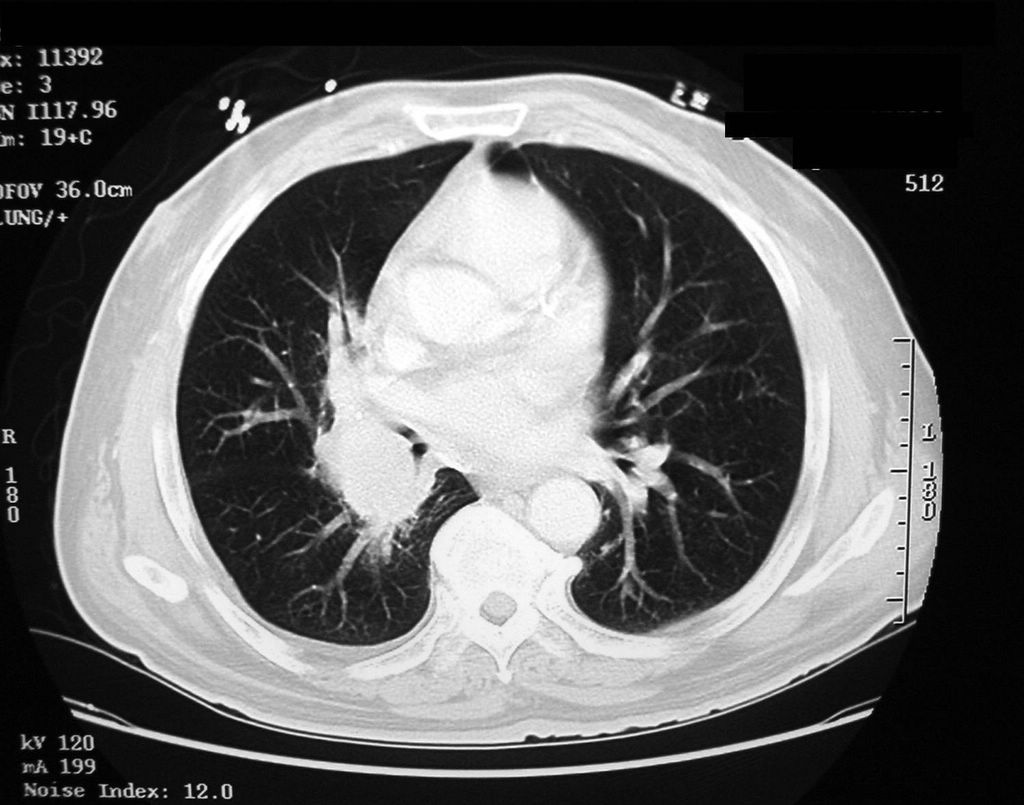
CT of the chest shows the RUL mass and mediastinal lymphadenopathy.



CT chest





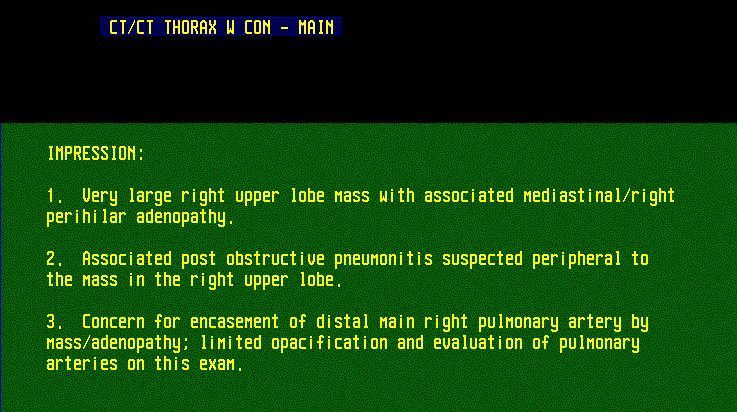
CT chest; CT report
CT report:
There is a large relatively hypodense mass involving much of the right upper lobe and directly abutting the superior mediastinum on the right. The appearance is highly suspicious for upper lobe neoplasm, possibly with associated post obstructive pneumonitis more peripherally. This mass is estimated to measure approximately 8.2 cm A.P. by 5.8 cm transversely while extending for approximately 10 cm cephalocaudally. There is massive mediastinal adenopathy, predominantly in the right paratracheal region. There is further extensive right perihilar adenopathy, not easily demarcated from mass.
There is mild narrowing of the right upper lobe bronchus. There is apparent encasement of the distal main right pulmonary artery by mass/adenopathy. This was not optimally defined on the current study, due to limited enhancement of the right pulmonary artery. Perihilar calcifications are noted bilaterally, suggesting old granulomatous disease. There is evidence of underlying emphysema.
There is a very small right pleural effusion.
What happened?
He was sent for bronchoscopy but at the beginning of the procedure, he refused and will be scheduled for a CT-guided transthoracic biopsy.

Antibiotic treatment for post-obstructive pneumonia
The CT-guided biopsy showed invasive poorly differentiated non-small cell carcinoma, consistent with poorly differentiated squamous cell carcinoma, tumor necrosis was present. The slides showed a long core of tissue, demonstrating invasive epithelial cell tumor without glandular differentiation. The tumor cells were large and polygonal with large hyperchromatic nuclei with frequent mitosis.
A CT scan of the abdomen and a whole body bone scan will be done for staging of the lung cancer.
Final diagnosis: Post-obstructive pneumonia. Lung cancer.
References:
Finger Clubbing in Merck Manual
Now, he complains of cough productive of yellow sputum for about one week, and reports some weight loss but he cannot say how much.
PMH: Smoker, EtOH abuse
Medications: none
SH: Smoker - 30 pck-yr, quit 2 weeks ago, drinks 1 pint of liquor per day
Physical examination: Thin man in NAD
VS 37.7-105-137/61-18.
Chest: breath sounds are reduced in the right upper lobe
CVS: Clear S1S2
Abdomen: Soft, NT, ND
Extremities: clubbing


Clubbing in a long-term smoker with suspected lung cancer
What do you think is going on?
Pneumonia?
TB?
Cancer?
What tests would you order?
CXR
CBCD, CMP
CBC shows anemia due to iron deficiency, malnutriton (note Alb level is 1.8), alcohol abuse and chronic disease
CXR
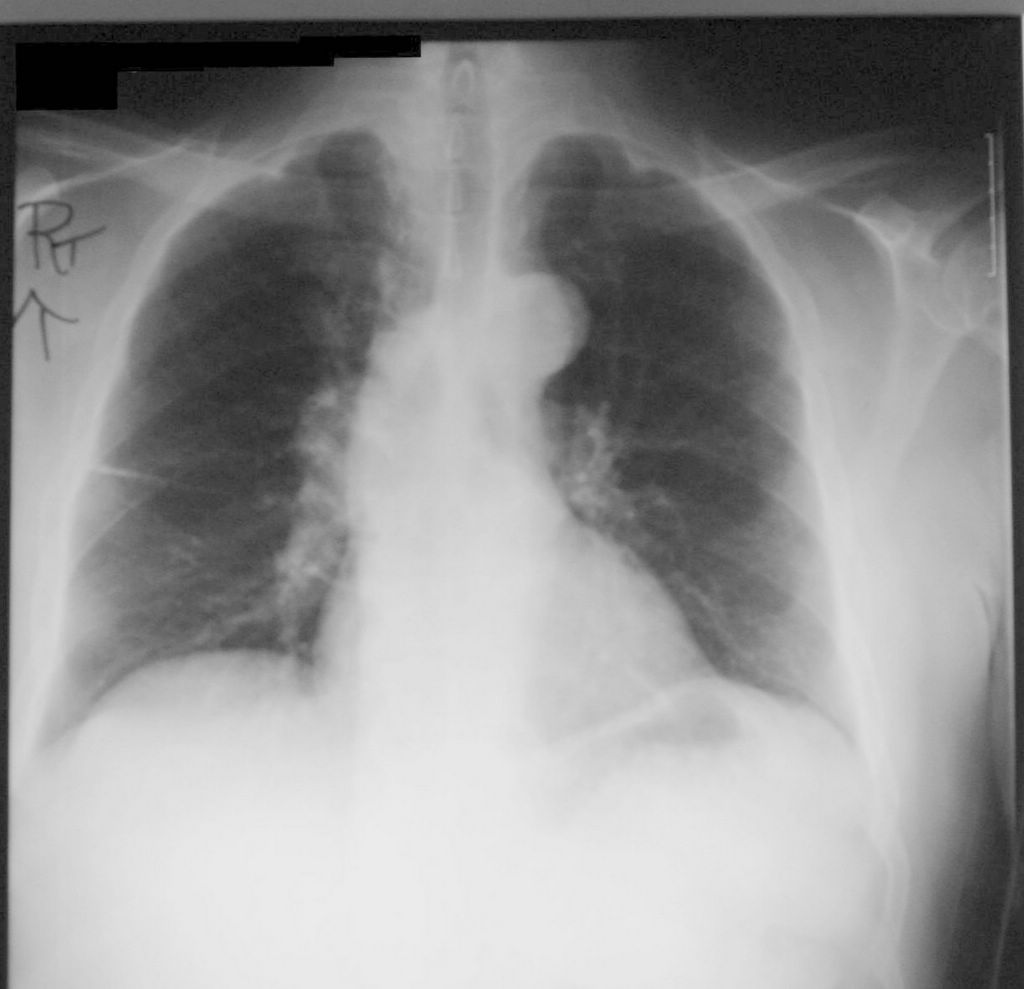

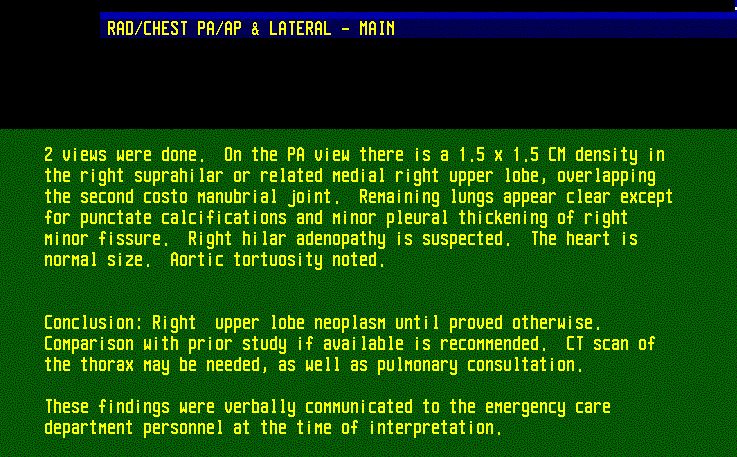
PA CXR showed a small RUL mass one year ago. The patient was advised to follow-up with his physician and to have a CT scan of the chest but he was drinking heavily at the time and he never followed up on the findings. Close-up of the RUL mass. Previous CXR report.
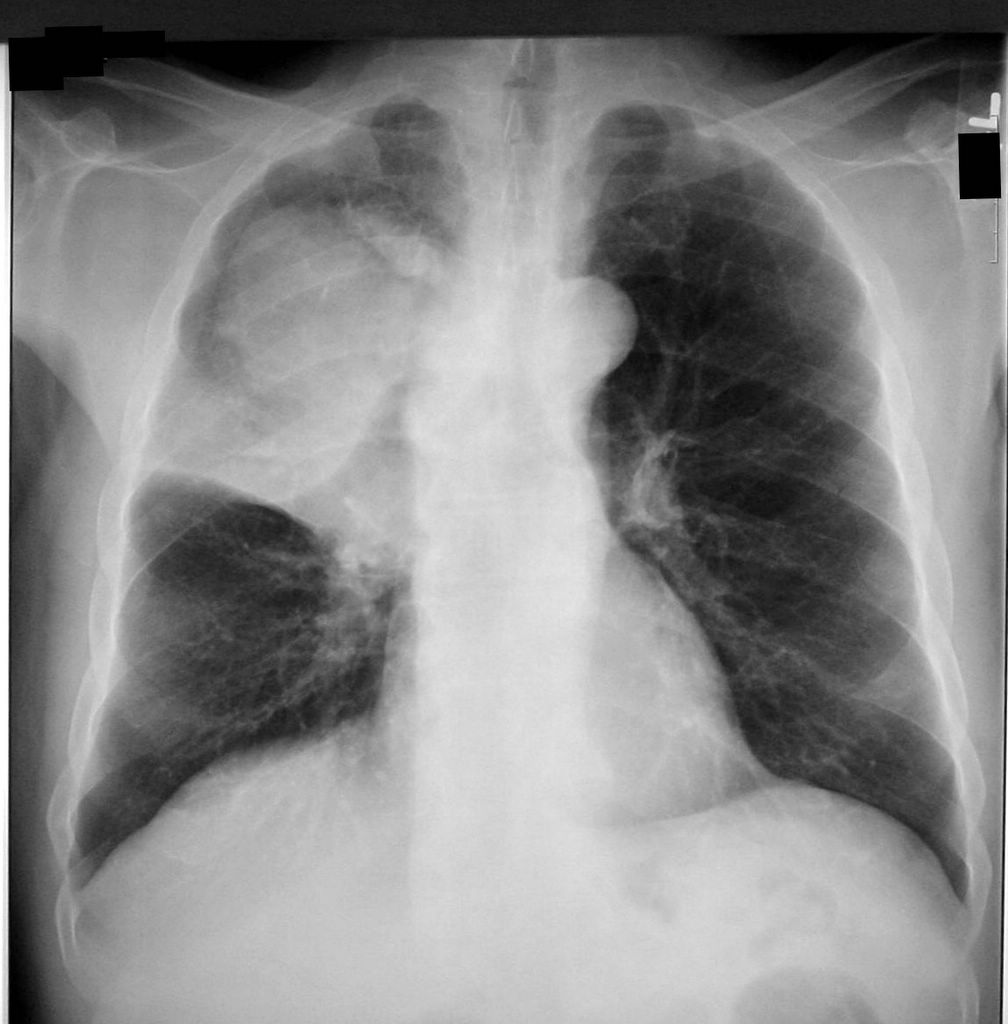

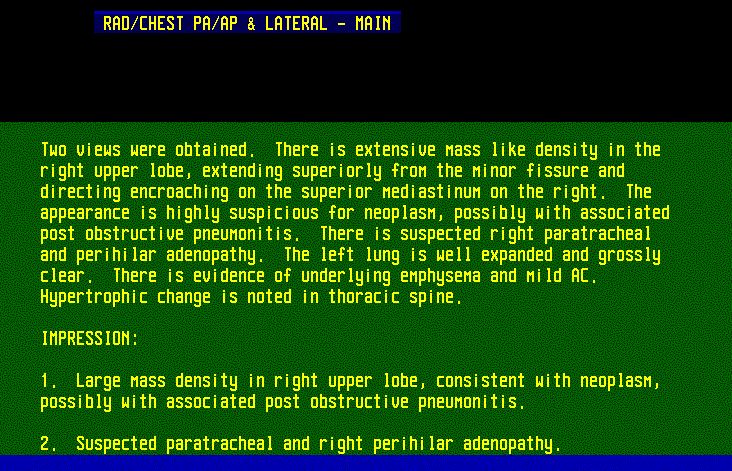
The RUL mass seen on the previous CXR one ago, has strikingly increased in size. Lateral film shows a large RUL mass. CXR report.
CT of the chest




CT of the chest shows the RUL mass and mediastinal lymphadenopathy.


CT chest



CT chest; CT report
CT report:
There is a large relatively hypodense mass involving much of the right upper lobe and directly abutting the superior mediastinum on the right. The appearance is highly suspicious for upper lobe neoplasm, possibly with associated post obstructive pneumonitis more peripherally. This mass is estimated to measure approximately 8.2 cm A.P. by 5.8 cm transversely while extending for approximately 10 cm cephalocaudally. There is massive mediastinal adenopathy, predominantly in the right paratracheal region. There is further extensive right perihilar adenopathy, not easily demarcated from mass.
There is mild narrowing of the right upper lobe bronchus. There is apparent encasement of the distal main right pulmonary artery by mass/adenopathy. This was not optimally defined on the current study, due to limited enhancement of the right pulmonary artery. Perihilar calcifications are noted bilaterally, suggesting old granulomatous disease. There is evidence of underlying emphysema.
There is a very small right pleural effusion.
What happened?
He was sent for bronchoscopy but at the beginning of the procedure, he refused and will be scheduled for a CT-guided transthoracic biopsy.

Antibiotic treatment for post-obstructive pneumonia
The CT-guided biopsy showed invasive poorly differentiated non-small cell carcinoma, consistent with poorly differentiated squamous cell carcinoma, tumor necrosis was present. The slides showed a long core of tissue, demonstrating invasive epithelial cell tumor without glandular differentiation. The tumor cells were large and polygonal with large hyperchromatic nuclei with frequent mitosis.
A CT scan of the abdomen and a whole body bone scan will be done for staging of the lung cancer.
Final diagnosis: Post-obstructive pneumonia. Lung cancer.
References:
Finger Clubbing in Merck Manual