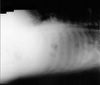
57 yo AAM is admitted to the hospital with CC: SOB for 2 weeks. The CXR shows a large left-side pleural effusion.

Massive left sided pleural effusion.
CXR report:
Findings: The lower two-thirds of the left chest is completely opacified probably due to a large pleural effusion. There is left lower lobe atelectasis. The right lung is clear. The pulmonary vascularity is normal. The cardiac silhouette is not well seen.
Impression: Large left pleural effusion with left lower lobe atelectasis. Follow up to complete resolution is necessary.
What else do you order for somebody with a pleural effusion?
A lateral decubitus film
Lateral decubitus film shows layering of the pleural effusion. The decubitus film is important for two reasons. First, it shows the size of the effusion - if the fluid layer is more than 1 cm, there is enough of it to do a pleural tap. Second, the decubitus film can reveal any loculations in the effusion which make the tap more difficult and are indication for a CT-guided thoracocentesis.
Lateral decubitus CXR report:
Indications: Shortness of breath for two weeks and left pleural effusion
Findings: Lateral decubitus views of the chest show near complete opacification of the left chest. The right chest appears clear. Compared to the upright PA view there appears to be layering of the left pleural effusion although due to the massive volume the meniscus is not well seen.
Impression: Huge left pleural effusion
What would you do?
He needs a thoracocentesis.
What happened?
A pleural tap was attempted but was unsuccessful and a CT-guided thoracocentesis was done.
The procedure was performed in the radiology department under local anesthesia.
Under sterile conditions and CT guidance, a 10 French pigtail catheter was introduced into the left pleural space. A total of approximately 2.8 l of amber colored fluid was drained. Specimens were forward to the lab for analysis as requested. The patient tolerated the procedure well and no immediate complications were noted. There was no sign of pneumothorax following the aspiration.


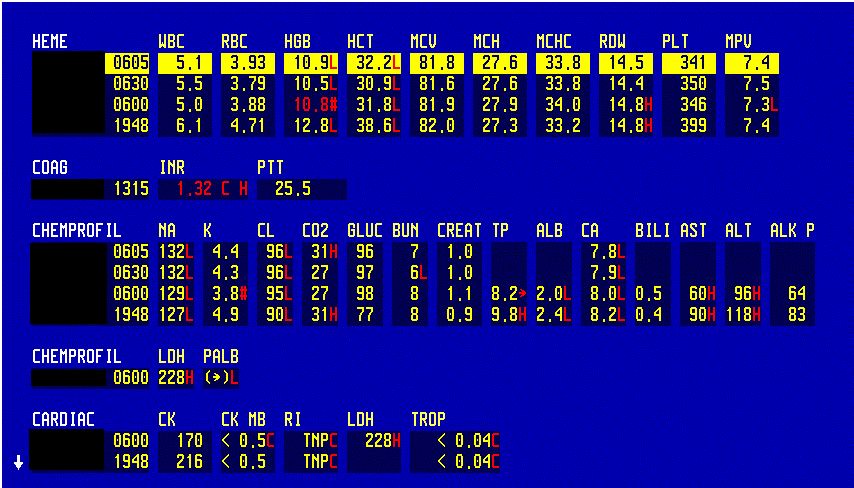
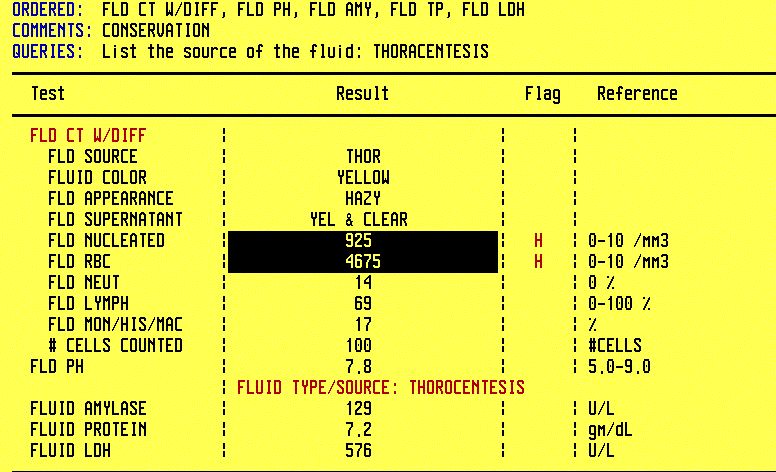
CBC and CMP; Effusion fluid analysis
How do you distinguish between exudate and transudate?
By using the classic Light's criteria for exudate - look at 3 values. An exudate has one or more of the following characteristics:
Pleural fluid serum protein ratio more than 0.5
7.2 / 8.2 = 0.87 (our case)
Pleural fluid serum LDH ratio more than 0.6
576 / 228 = 2.52
Pleural fluid LDH more than two thirds of normal serum value
Yes
New simplified criteria:
Pleural fluid LDH more than 0.45 of the upper limit of normal serum values .
Yes
Pleural fluid cholesterol more than 45 mg/dL.
Not measured
Pleural fluid protein more than 2.9 g/dL.
7.2
ABx Treatment
Final diagnosis: Massive Left-Sided Pleural Effusion
References:
Pleural Effusion - eMedicine

Massive left sided pleural effusion.
CXR report:
Findings: The lower two-thirds of the left chest is completely opacified probably due to a large pleural effusion. There is left lower lobe atelectasis. The right lung is clear. The pulmonary vascularity is normal. The cardiac silhouette is not well seen.
Impression: Large left pleural effusion with left lower lobe atelectasis. Follow up to complete resolution is necessary.
What else do you order for somebody with a pleural effusion?
A lateral decubitus film

Lateral decubitus film shows layering of the pleural effusion. The decubitus film is important for two reasons. First, it shows the size of the effusion - if the fluid layer is more than 1 cm, there is enough of it to do a pleural tap. Second, the decubitus film can reveal any loculations in the effusion which make the tap more difficult and are indication for a CT-guided thoracocentesis.
Lateral decubitus CXR report:
Indications: Shortness of breath for two weeks and left pleural effusion
Findings: Lateral decubitus views of the chest show near complete opacification of the left chest. The right chest appears clear. Compared to the upright PA view there appears to be layering of the left pleural effusion although due to the massive volume the meniscus is not well seen.
Impression: Huge left pleural effusion
What would you do?
He needs a thoracocentesis.
What happened?
A pleural tap was attempted but was unsuccessful and a CT-guided thoracocentesis was done.
The procedure was performed in the radiology department under local anesthesia.
Under sterile conditions and CT guidance, a 10 French pigtail catheter was introduced into the left pleural space. A total of approximately 2.8 l of amber colored fluid was drained. Specimens were forward to the lab for analysis as requested. The patient tolerated the procedure well and no immediate complications were noted. There was no sign of pneumothorax following the aspiration.
CBC and CMP; Effusion fluid analysis
How do you distinguish between exudate and transudate?
By using the classic Light's criteria for exudate - look at 3 values. An exudate has one or more of the following characteristics:
Pleural fluid serum protein ratio more than 0.5
7.2 / 8.2 = 0.87 (our case)
Pleural fluid serum LDH ratio more than 0.6
576 / 228 = 2.52
Pleural fluid LDH more than two thirds of normal serum value
Yes
New simplified criteria:
Pleural fluid LDH more than 0.45 of the upper limit of normal serum values .
Yes
Pleural fluid cholesterol more than 45 mg/dL.
Not measured
Pleural fluid protein more than 2.9 g/dL.
7.2
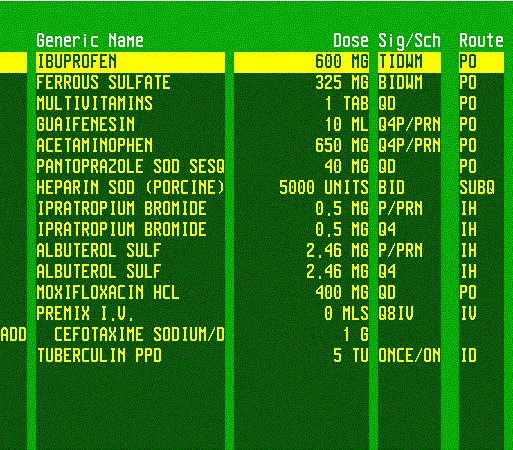
ABx Treatment
Final diagnosis: Massive Left-Sided Pleural Effusion
References:
Pleural Effusion - eMedicine