Case scenario:
A 65-year-old Caucasian female (CF) has a new-onset dysphagia secondary to stroke. The speech therapist did a swallow evaluation and found out that the patient is at high risk for aspiration even with soft mechanical diet and honey-thick liquids. She recommended placing a fine-bore feeding tube, Isocal HN with a goal of 90 ml/hr and a repeat swallow evaluation in 3-4 days.
The patient understands and agrees. You have just placed a Corpak tube and tested its postion by pushing 30 cc of air through the tube.
How to confirm the nasogastric tube (NGT) placement? By CXR or KUB?
NGT placement is confirmed by CXR. It is important to see that the NGT is below the diaphragm. One JAMA report concluded that the traditional physical examination-based methods of assessing proper NGT placement are inadequate when applied to the small-bore tubes (for example, Corpak). Only a CXR can assure placement in the stomach.
Why not KUB? What are the complications of NGT placement?
Most of the important complications of NGT placement are related to penetrating the esophagus or passing the tube in the trachea and bronchi. Occasionally, an NGT can penetrate the brain. These misplacements will not be shown on the abdominal x-ray (KUB) and the consequences can be deadly:
In 2000, a 78 year old patient died after she was fed through an NGT which was wrongly placed. The prosecutor case was that the junior doctor had been asked by nurses to look at an x-ray that would have shown that the tube was protruding into a lung and had given the go ahead for feeding to start. When the patient was fed, the food passed into her lung, and she died from acute pneumonia (Source: BMJ 2003).
Examples of NGT misplacement:

NGT in right main bronchus. Report of KUB/Abdomen - portable: A Corpak feeding tube is in place with the tip extending into the right mainstem bronchus. The staff was aware and the feeding tube had been pulled. There is no bowel obstruction.
This X-ray clearly shows why NGT placement should be confirmed with CXR. KUB almost missed the NGT tip.

NGT is too high, in the esophagus and above the diaphragm, not in the stomach. This placement is associated with high risk for aspiration. The NGT must be advanced further down and the new placement should be confirmed with a CXR.
Some important things to remember:

- Measure the expected lenght to reach the stomach (the suggested method is shown here, image source: CPEM.org)
- Sit the patient upright, if possible
- Flex the neck a little. This is just the opposite of the neck extension which is essential for tracheal intubation. In NGT placement you want to avoid the tracheal intubation. This is the reason for flexing the neck.
- Never force the NGT, it should go down smoothly. Ask the patient to swallow.
- Read more about the procedure in the references listed below
If you are not sucessful in placing an NGT on the first attempt, do not despair. Ask somebody (a senior colleague) to help you. Even Dr. Genes, the founder of the online Grand Rounds, had trouble passing a NGT as an intern.
References
Nasogastric Intubation. NEJM Videos in Clinical Medicine.
Pneumothorax complicating small-bore feeding tube placement - JAMA 3/1991
Thoracic complications of nasogastric tube: review of safe practice - Interact CardioVasc Thorac Surg 2005
Nasogastric tube insertion - Department of Emergency Medicine, University of Ottawa
Junior doctor is cleared of manslaughter after feeding tube error - BMJ 2003
The accidental introduction of the nasogastric tube into the brain. Case report. Acta Chir Scand. 1978
Blueprints Clinical Procedures - Google Book Search
Handbook of Gastroenterologic Procedures - Google Book Search
Core Clinical Skills: How to Succeed in Osces in Medicine - Google Book Search
Practical Procedures (PDF, 500 kb) - FleshandBones.com
Insert a Nasogastric Tube - Naval Medical Center, Portsmouth
Assessing placement of feeding tubes. Am J Nurs. 2001 May (subscription required)
Procedure guidelines: Nasogastric intubation with tubes using an introducer
Insertion of NGT - ICU Procedure Manual - medicineau.net.au
Nasogastric Intubation - MedicineClinic.org
Practical procedures - WHO
Insertion and management of fine bore feeding tubes - Leeds Hospital
Doctors feed Pope by nasal tube - BBC News
Read more about dysphagia and diets - ahrq.gov, cedwvu.org, gicare.com
Image source: CPEM.org
A 65-year-old Caucasian female (CF) has a new-onset dysphagia secondary to stroke. The speech therapist did a swallow evaluation and found out that the patient is at high risk for aspiration even with soft mechanical diet and honey-thick liquids. She recommended placing a fine-bore feeding tube, Isocal HN with a goal of 90 ml/hr and a repeat swallow evaluation in 3-4 days.
The patient understands and agrees. You have just placed a Corpak tube and tested its postion by pushing 30 cc of air through the tube.
How to confirm the nasogastric tube (NGT) placement? By CXR or KUB?
NGT placement is confirmed by CXR. It is important to see that the NGT is below the diaphragm. One JAMA report concluded that the traditional physical examination-based methods of assessing proper NGT placement are inadequate when applied to the small-bore tubes (for example, Corpak). Only a CXR can assure placement in the stomach.
Why not KUB? What are the complications of NGT placement?
Most of the important complications of NGT placement are related to penetrating the esophagus or passing the tube in the trachea and bronchi. Occasionally, an NGT can penetrate the brain. These misplacements will not be shown on the abdominal x-ray (KUB) and the consequences can be deadly:
In 2000, a 78 year old patient died after she was fed through an NGT which was wrongly placed. The prosecutor case was that the junior doctor had been asked by nurses to look at an x-ray that would have shown that the tube was protruding into a lung and had given the go ahead for feeding to start. When the patient was fed, the food passed into her lung, and she died from acute pneumonia (Source: BMJ 2003).
Examples of NGT misplacement:
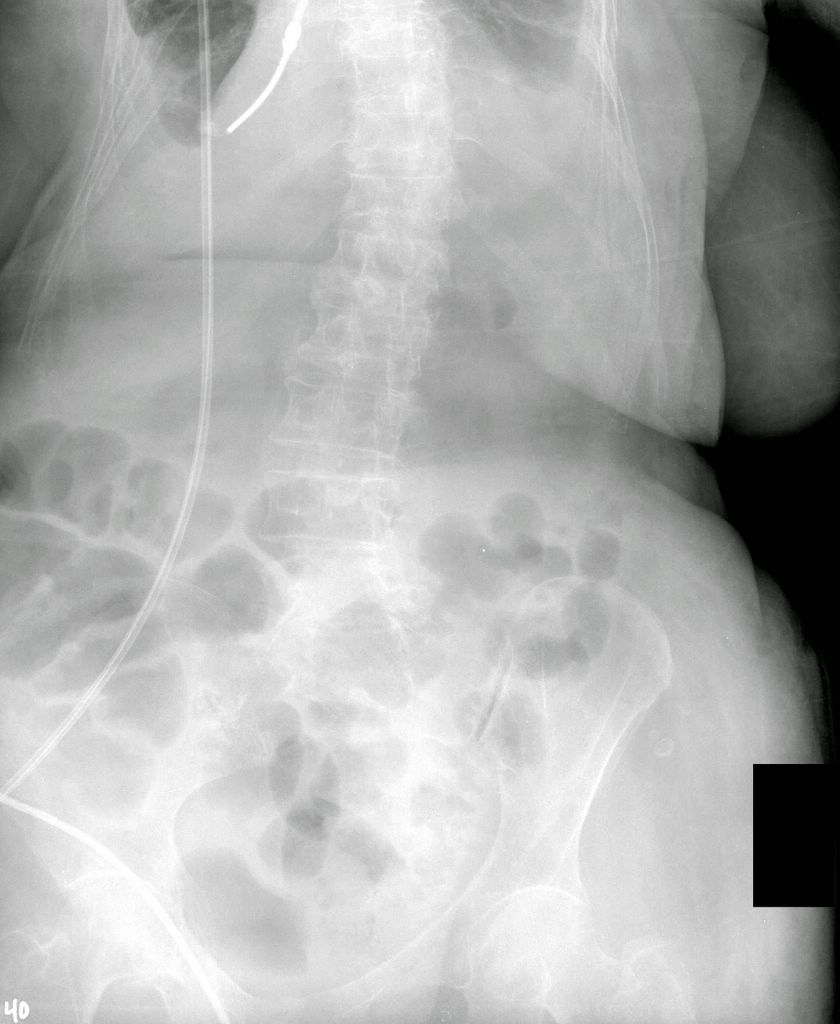
NGT in right main bronchus. Report of KUB/Abdomen - portable: A Corpak feeding tube is in place with the tip extending into the right mainstem bronchus. The staff was aware and the feeding tube had been pulled. There is no bowel obstruction.
This X-ray clearly shows why NGT placement should be confirmed with CXR. KUB almost missed the NGT tip.
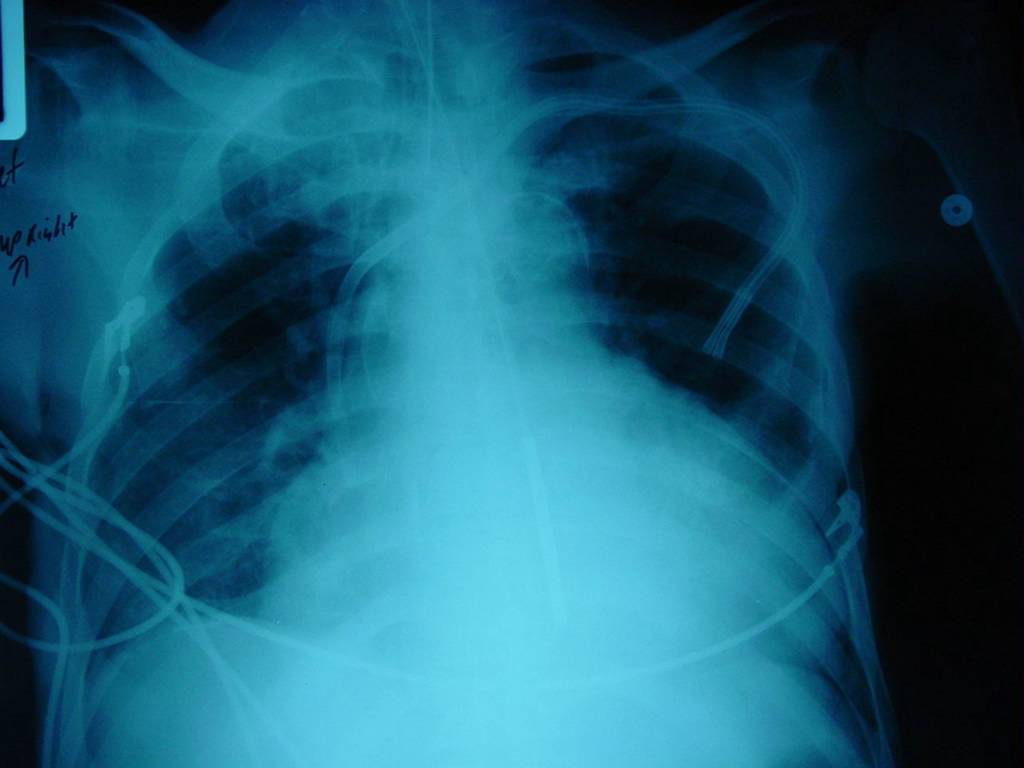
NGT is too high, in the esophagus and above the diaphragm, not in the stomach. This placement is associated with high risk for aspiration. The NGT must be advanced further down and the new placement should be confirmed with a CXR.
Some important things to remember:
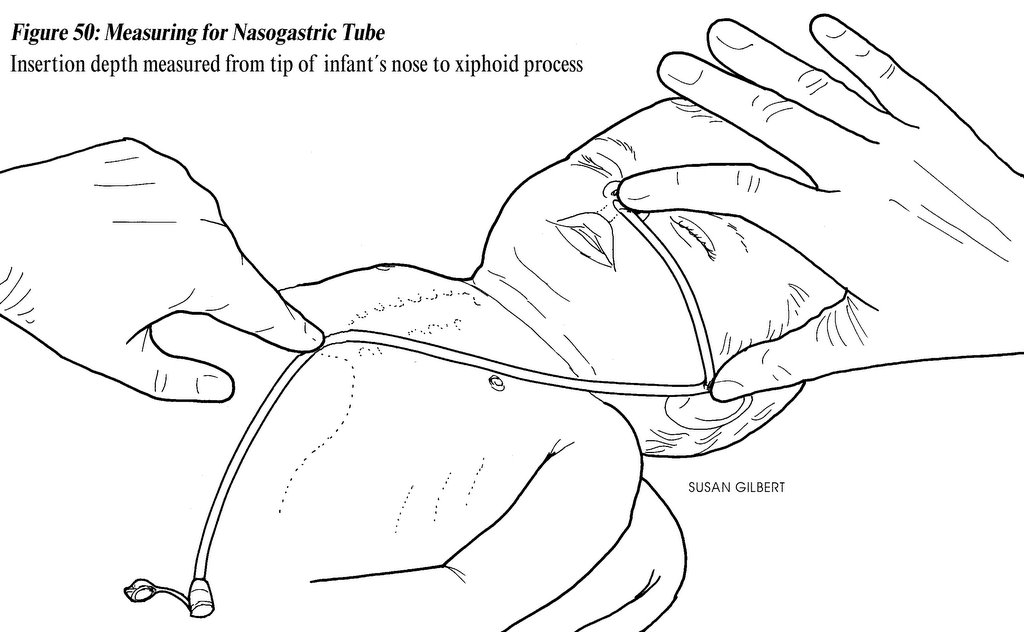
- Measure the expected lenght to reach the stomach (the suggested method is shown here, image source: CPEM.org)
{kind=link}
- Sit the patient upright, if possible
- Flex the neck a little. This is just the opposite of the neck extension which is essential for tracheal intubation. In NGT placement you want to avoid the tracheal intubation. This is the reason for flexing the neck.
- Never force the NGT, it should go down smoothly. Ask the patient to swallow.
- Read more about the procedure in the references listed below
If you are not sucessful in placing an NGT on the first attempt, do not despair. Ask somebody (a senior colleague) to help you. Even Dr. Genes, the founder of the online Grand Rounds, had trouble passing a NGT as an intern.
References
Nasogastric Intubation. NEJM Videos in Clinical Medicine.
Pneumothorax complicating small-bore feeding tube placement - JAMA 3/1991
Thoracic complications of nasogastric tube: review of safe practice - Interact CardioVasc Thorac Surg 2005
Nasogastric tube insertion - Department of Emergency Medicine, University of Ottawa
Junior doctor is cleared of manslaughter after feeding tube error - BMJ 2003
The accidental introduction of the nasogastric tube into the brain. Case report. Acta Chir Scand. 1978
Blueprints Clinical Procedures - Google Book Search
Handbook of Gastroenterologic Procedures - Google Book Search
Core Clinical Skills: How to Succeed in Osces in Medicine - Google Book Search
Practical Procedures (PDF, 500 kb) - FleshandBones.com
Insert a Nasogastric Tube - Naval Medical Center, Portsmouth
Assessing placement of feeding tubes. Am J Nurs. 2001 May (subscription required)
Procedure guidelines: Nasogastric intubation with tubes using an introducer
Insertion of NGT - ICU Procedure Manual - medicineau.net.au
Nasogastric Intubation - MedicineClinic.org
Practical procedures - WHO
Insertion and management of fine bore feeding tubes - Leeds Hospital
Doctors feed Pope by nasal tube - BBC News
Read more about dysphagia and diets - ahrq.gov, cedwvu.org, gicare.com
Image source: CPEM.org