 Small-cell lung cancer
Small-cell lung cancerDiagnosis relies on histology, with the use of immunohistochemical studies to confirm difficult cases.
Typical patients are men older than 70 years who are current or past heavy smokers and who have pulmonary and cardiovascular comorbidities.
Patients often present with rapid-onset symptoms due to:
- local intrathoracic tumour growth
- extrapulmonary distant spread
- paraneoplastic syndromes
- a combination of these features
Staging aims ultimately to define disease as metastatic or non-metastatic:
- Combination chemotherapy (platinum-based plus etoposide or irinotecan) is the mainstay first-line treatment for metastatic small-cell lung cancer.
- For non-metastatic disease, early concurrent thoracic radiotherapy is indicated.
Prophylactic cranial irradiation should be considered for all patients, even without metastases, whose disease does not progress after induction chemotherapy and radiotherapy.
Despite high initial response rates, most patients eventually relapse. Except for topotecan, few treatment options then remain.
Non-small-cell lung cancer (NSCLC)
The recently introduced 7th edition of the TNM classification relates better to other prognostic factors such as biological markers.
The advances in treatment include:
- a new generation of chemotherapy agents
- a proven advantage to adjuvant chemotherapy after complete resection for specific stage groups
- new techniques for radiotherapy
- new surgical approaches
References:
Small-cell lung cancer. The Lancet, Volume 378, Issue 9804, Pages 1741 - 1755, 12 November 2011
Non-small-cell lung cancer. The Lancet, Volume 378, Issue 9804, Pages 1727 - 1740, 12 November 2011
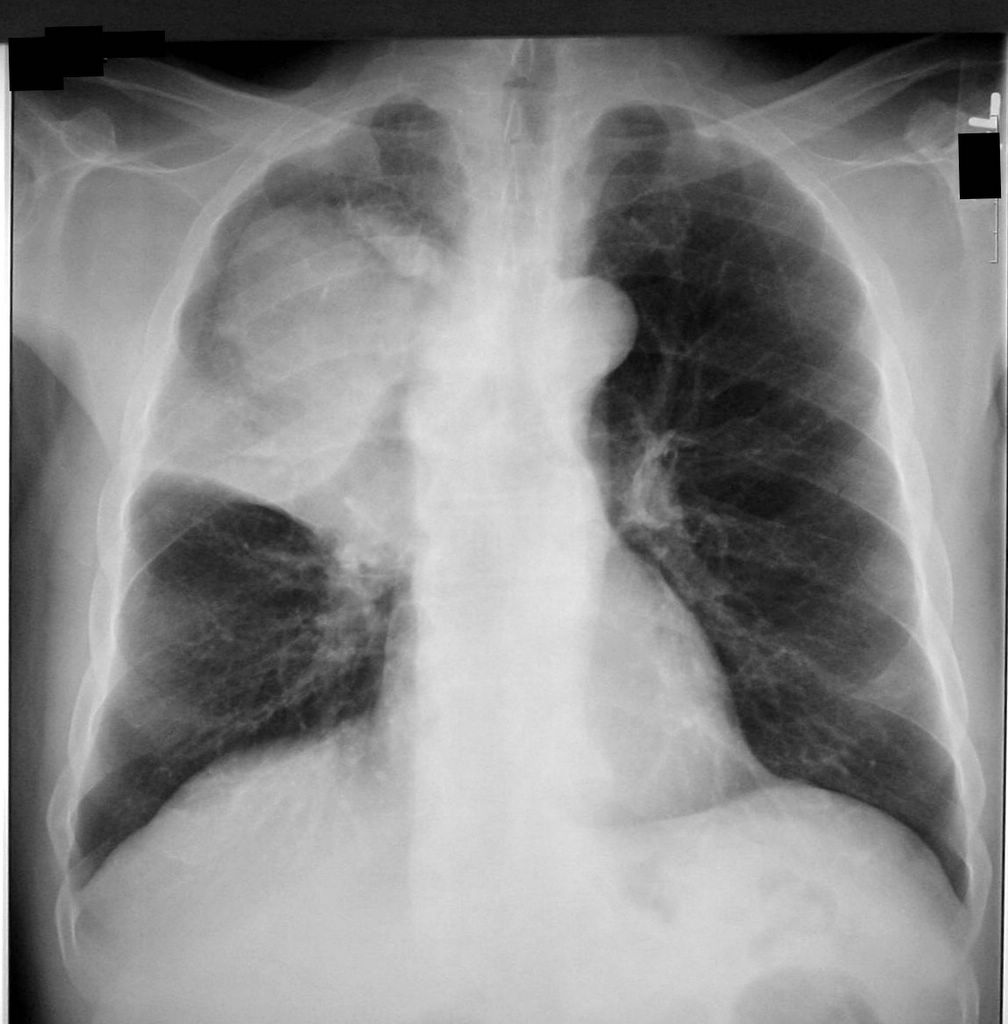
Image source: A CXR shows a right upper lobe (RUL) mass due to lung cancer. Source: Finger Clubbing due to Lung Cancer. Clinical Cases and Images.