57 yo AAM is admitted to the hospital with CC: SOB for 3-4 days. He is confused and c/o cough productive of yellow sputum. He remembers falling 4 times over the last 3 weeks without loosing consciousness. In the ER the patient was very tachypneic and hypoxic and was intubated.
CXR showed right lung opacification.
What is the reason?
Pneumonia?
Effusion?
Atelectasis?
CXR


Right lung atelectasis with mediastinal shift. ETT ends at the level of clavicles. The optimal position is in the middle between the clavicles and the carina. This ETT needs to be advanced 2 cm.
What happened?
CXR showed right lung atelectasis with multiple rib fractures bilaterally.
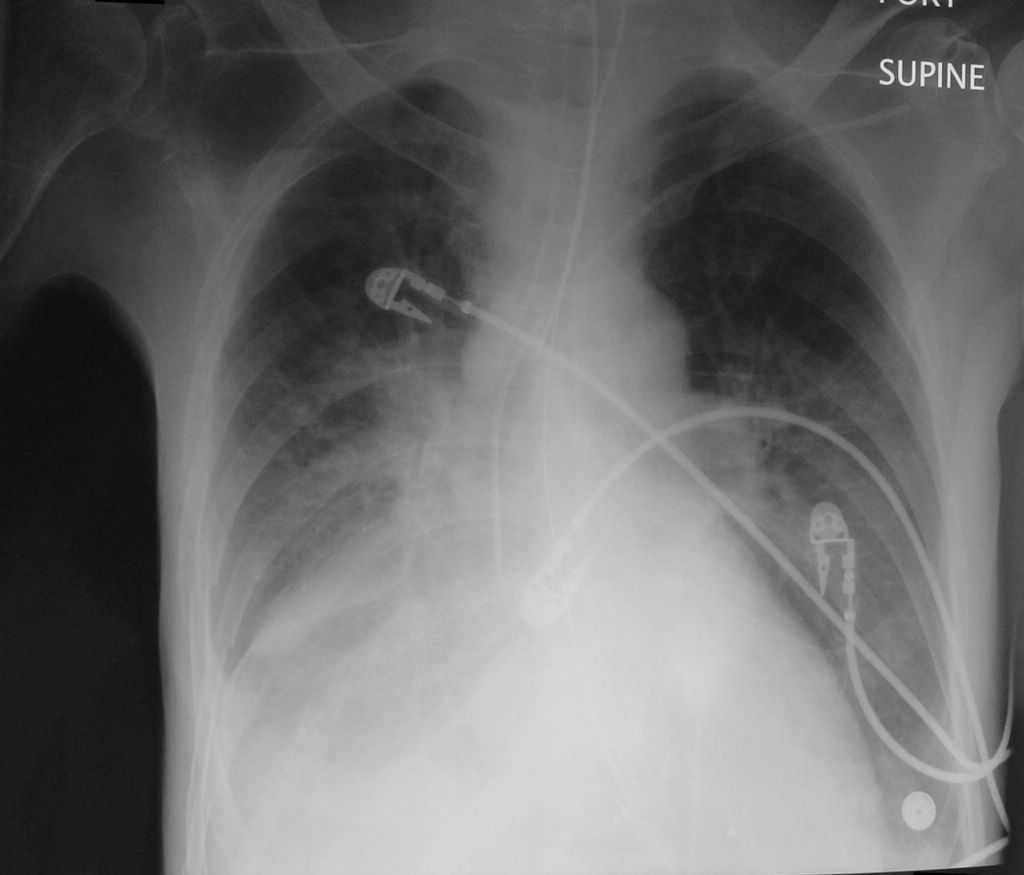
The patient had a lot of secretions and after suctioning, the oxygenation improved. CXR showed resolution of the right lung atelectasis.
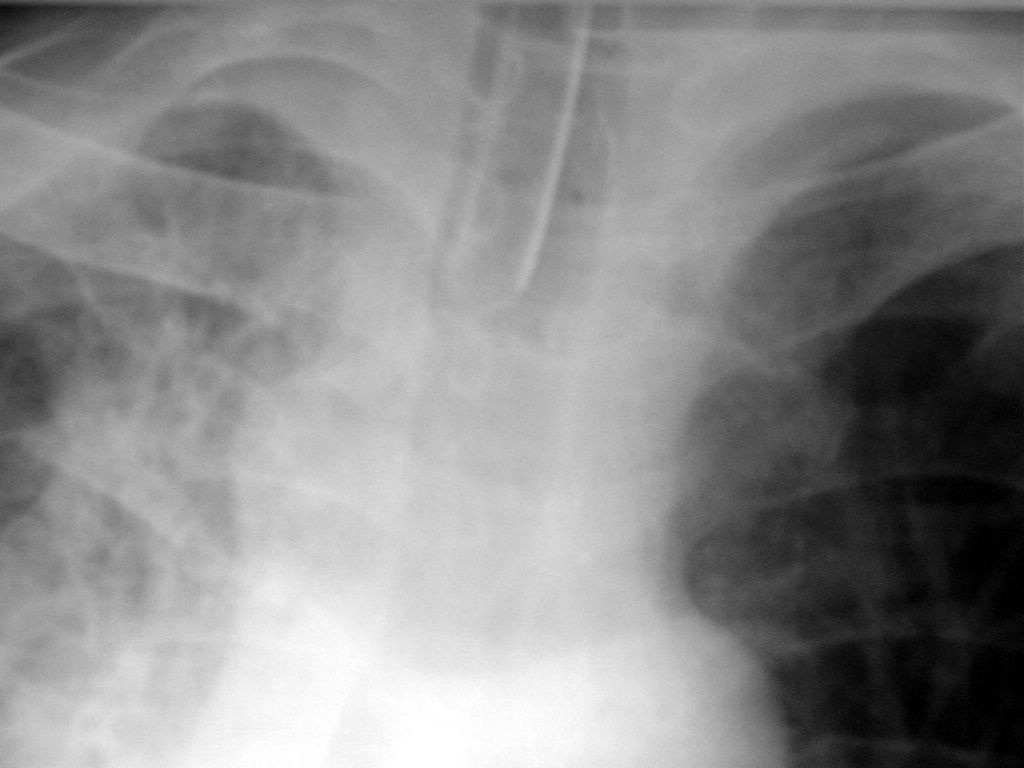
Note the position of the trachea on the CXR. The ETT is very close to the right bronchus and needs to be pulled out 2-3 cm.


Reexpansion of the right lung after suctioning and Mucomyst aerosols. The ETT is at the level of the right main bronchus and needs to be pulled back 2-3 cm.

Close-up of the right-sided rib fractures.
Final diagnosis: Right lung atelectasis. Bilateral pneumonia. Bilateral rib fractures.
What did we learn from this case?
The sequence of events was falls, multiple rib fractures, hypoventilation, atelectasis, pneumonia and respiratory failure.
Atelectasis is a common cause of lung opacification. It pulls the trachea and the mediastinum to its side. The pneumonia does not change the position of the mediastinal structures. A large pleural effusion can push the mediastinum to the opposite side.
Also note the size of the intercostal spaces and compare the left and right side. The intercostal spaces are diminished in atelectasis and may be widened with a large pleural effusion and pneumothorax.
CXR showed right lung opacification.
What is the reason?
Pneumonia?
Effusion?
Atelectasis?
CXR
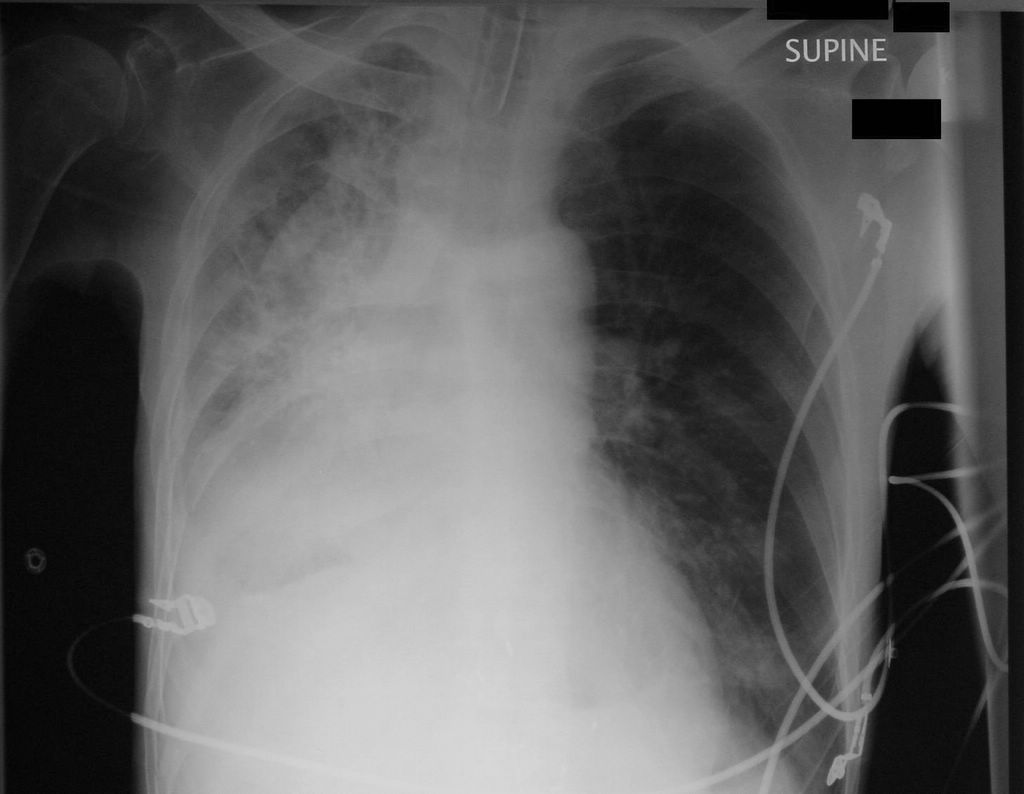
Right lung atelectasis with mediastinal shift. ETT ends at the level of clavicles. The optimal position is in the middle between the clavicles and the carina. This ETT needs to be advanced 2 cm.
What happened?
CXR showed right lung atelectasis with multiple rib fractures bilaterally.
The patient had a lot of secretions and after suctioning, the oxygenation improved. CXR showed resolution of the right lung atelectasis.
Note the position of the trachea on the CXR. The ETT is very close to the right bronchus and needs to be pulled out 2-3 cm.

Reexpansion of the right lung after suctioning and Mucomyst aerosols. The ETT is at the level of the right main bronchus and needs to be pulled back 2-3 cm.

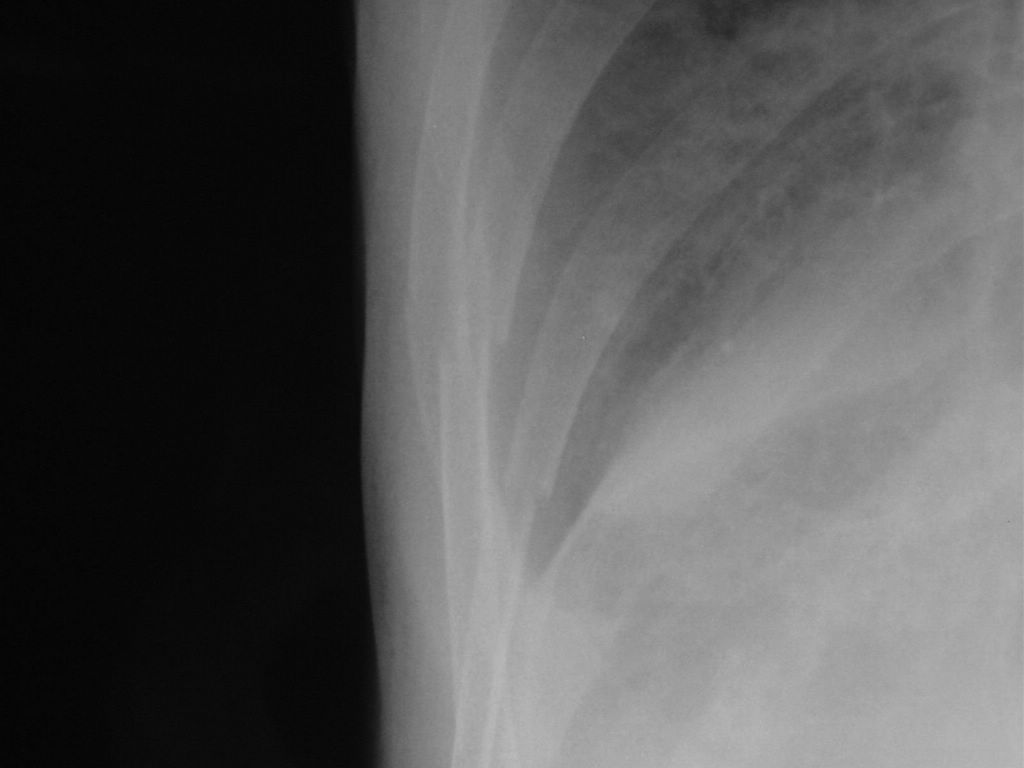
Close-up of the right-sided rib fractures.
Final diagnosis: Right lung atelectasis. Bilateral pneumonia. Bilateral rib fractures.
What did we learn from this case?
The sequence of events was falls, multiple rib fractures, hypoventilation, atelectasis, pneumonia and respiratory failure.
Atelectasis is a common cause of lung opacification. It pulls the trachea and the mediastinum to its side. The pneumonia does not change the position of the mediastinal structures. A large pleural effusion can push the mediastinum to the opposite side.
Also note the size of the intercostal spaces and compare the left and right side. The intercostal spaces are diminished in atelectasis and may be widened with a large pleural effusion and pneumothorax.