52 yo AAM is admitted to the hospital with CC: SOB and wheezing for 4 days. He has cough productive of clear white sputum and denies any fever or chills. He has a life-long history of asthma and says that he is compliant with his asthma inhalers. The patient was also diagnosed with sarcoidosis several years ago. He had a bronchoscopy and biopsy at that time which "did not show cancer".
PMH: Asthma/COPD, Sarcoidosis, HTN
Medications: Advair, inhalers, Lisinopril, HCTZ
SH: Former smoker
Physical examination:
VS 36.4-20-82-140/82
SpO2 98% on RA
Chest: decreased AE (B), wheezing (B)
CVS: Clear S1S2
Abdomen: Soft, NT, ND
Extremities: no c/c/e
What do you think is going on?
A typical asthma exacerbation?
Sarcoidosis flare-up?
Pneumonia?
Or something else?
What tests would you order?
CXR
CBCD, CMP
Sputum Gram stain, C+S
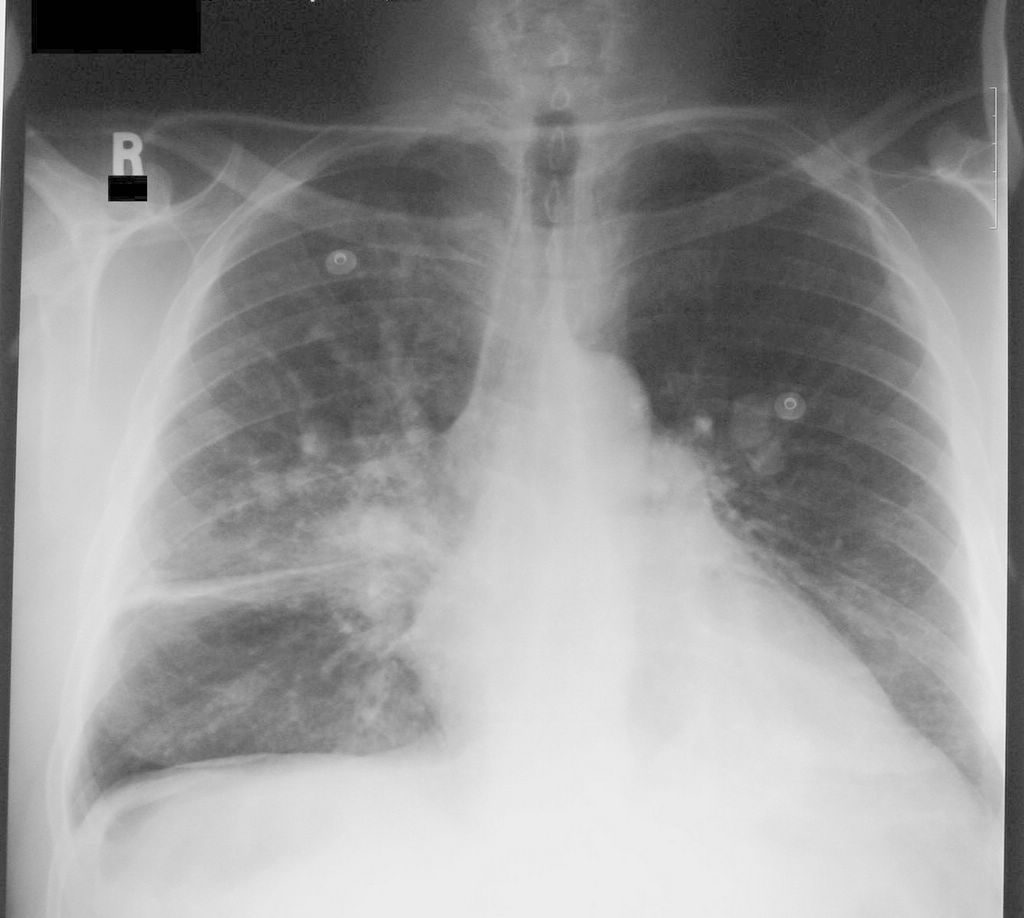
CXR


CXR two years ago. Close-up of the RLL.
CXR report: Since 2 years ago, limited portable upright view shows stable partially calcified hilar lymph nodes, pleural thickening of right minor fissure, the normal size heart. Previously demonstrated retrocardiac hiatus hernia is partly seen as a double density through the heart.


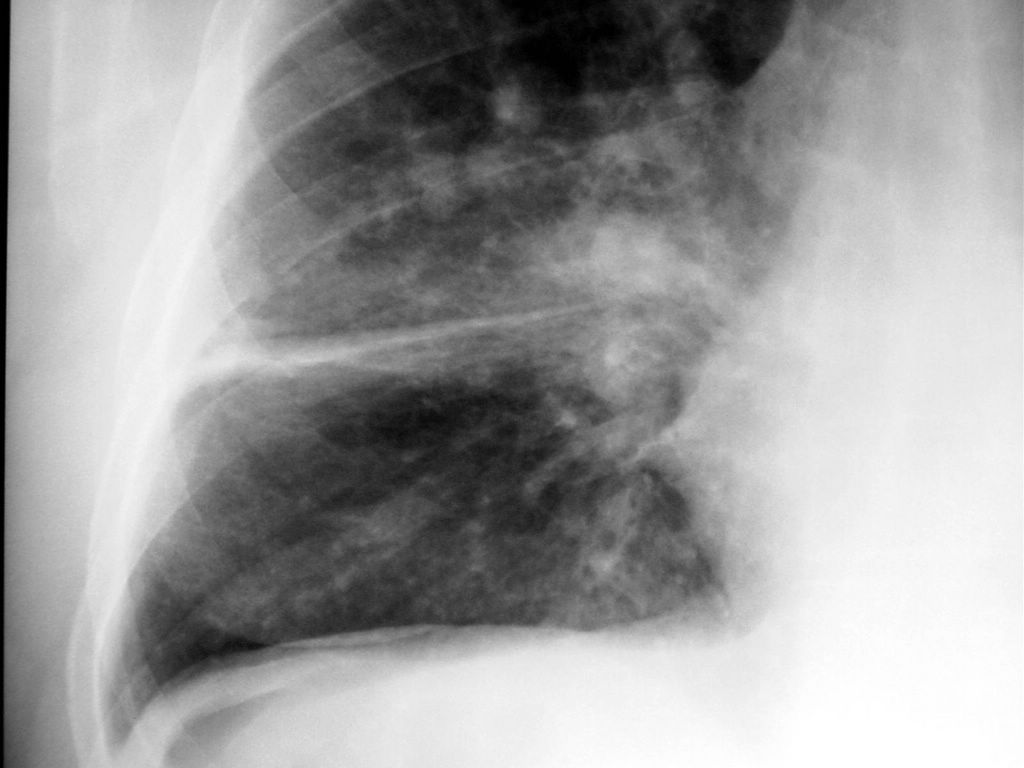
CXR on this admission; lateral CXR; report
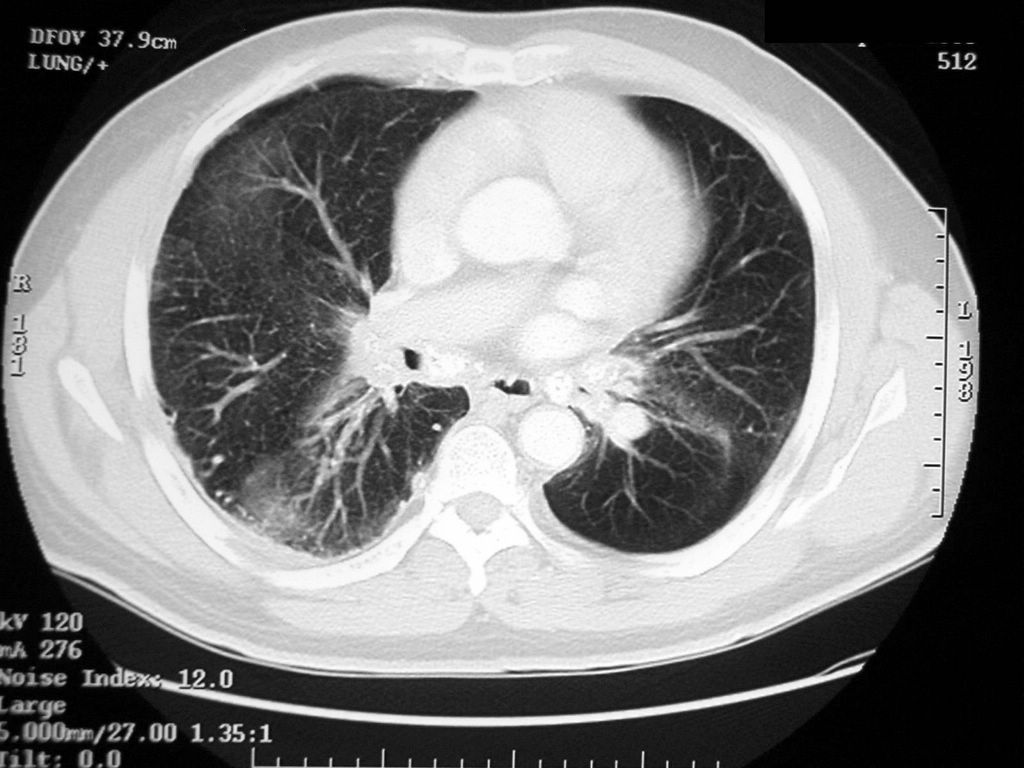
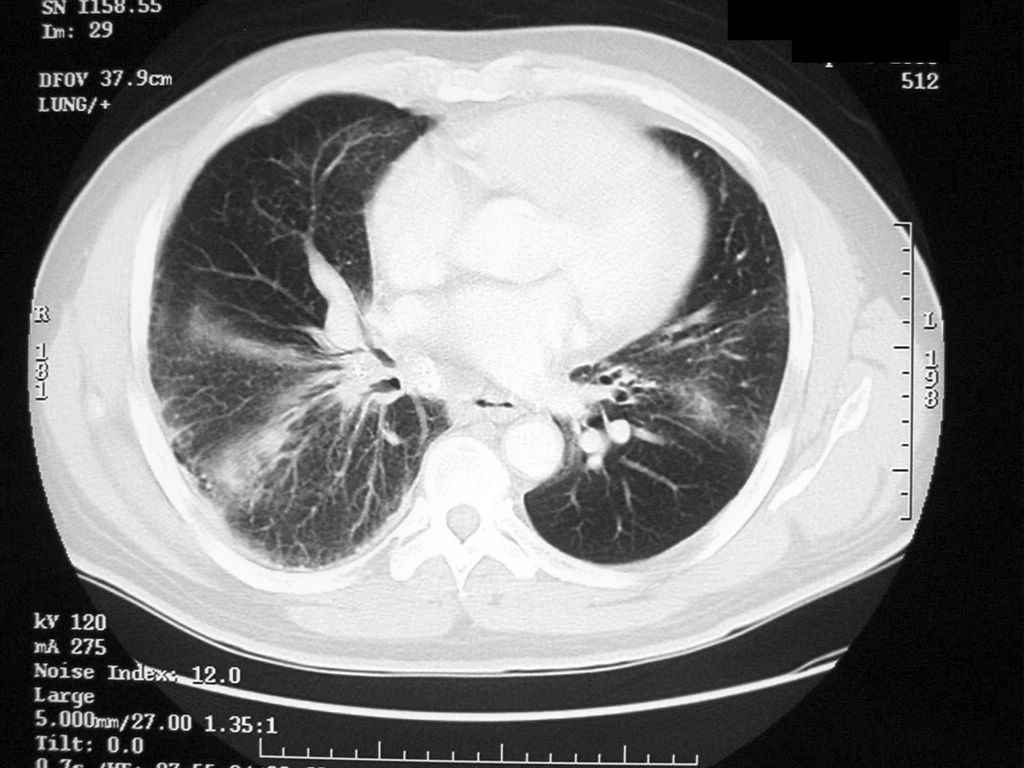
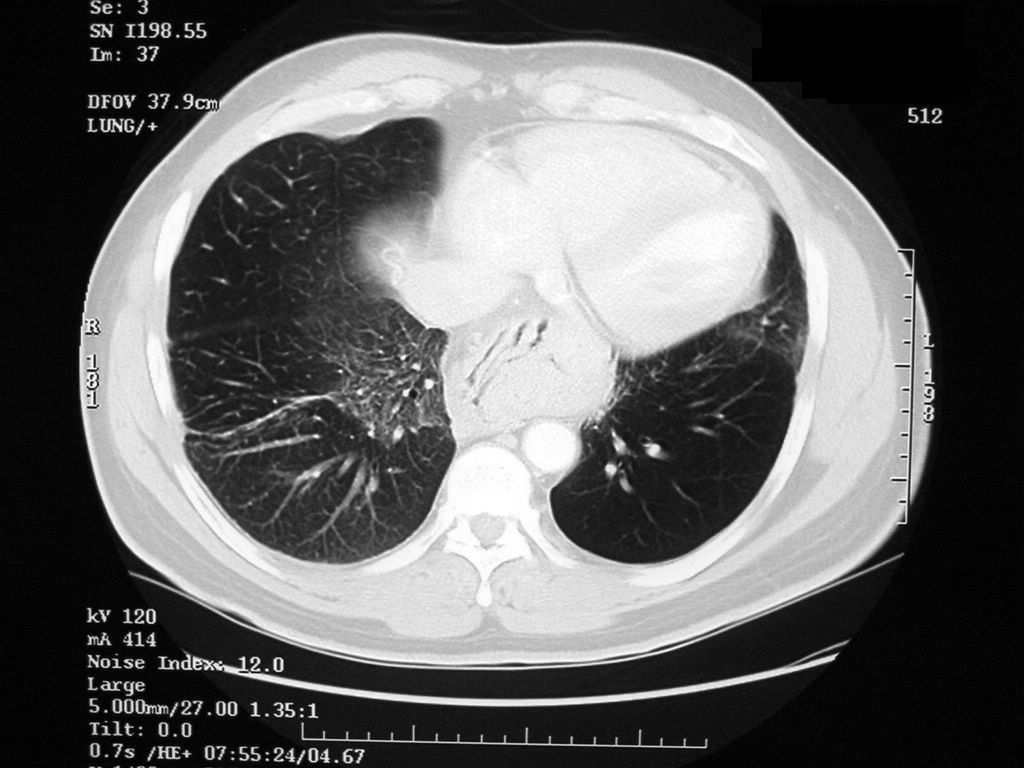
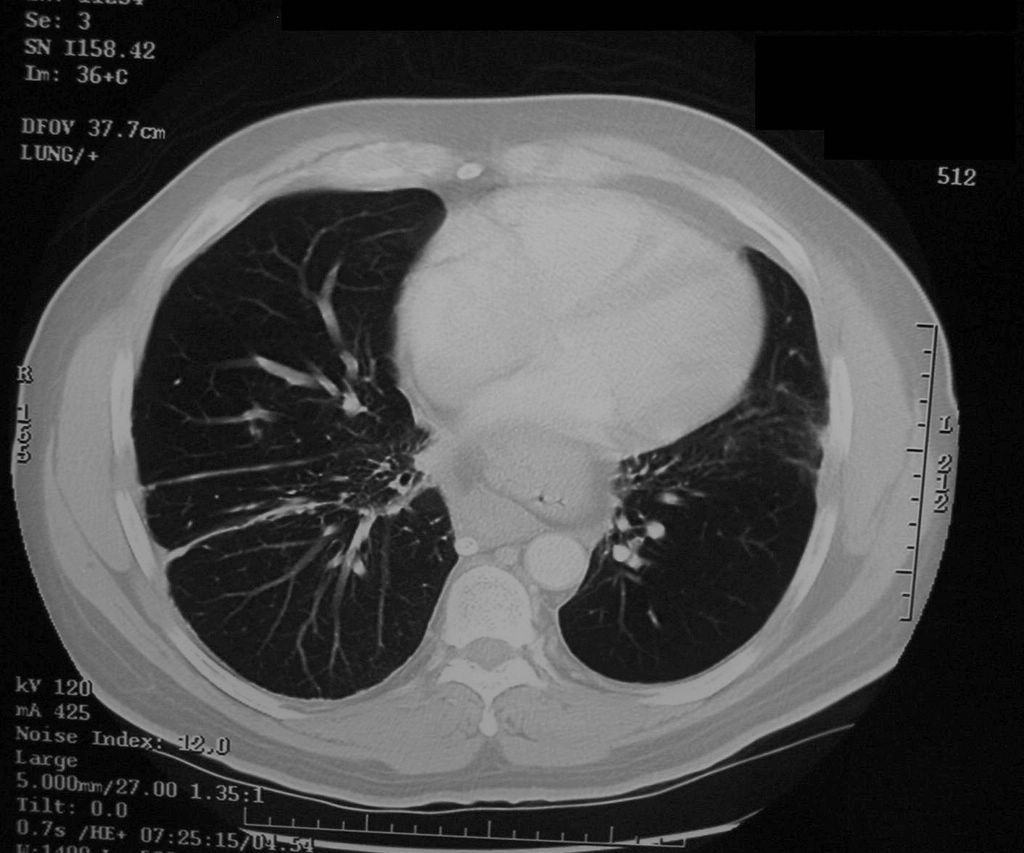
He also had a CT scan of the chest which showed diffuse ground glass pattern.



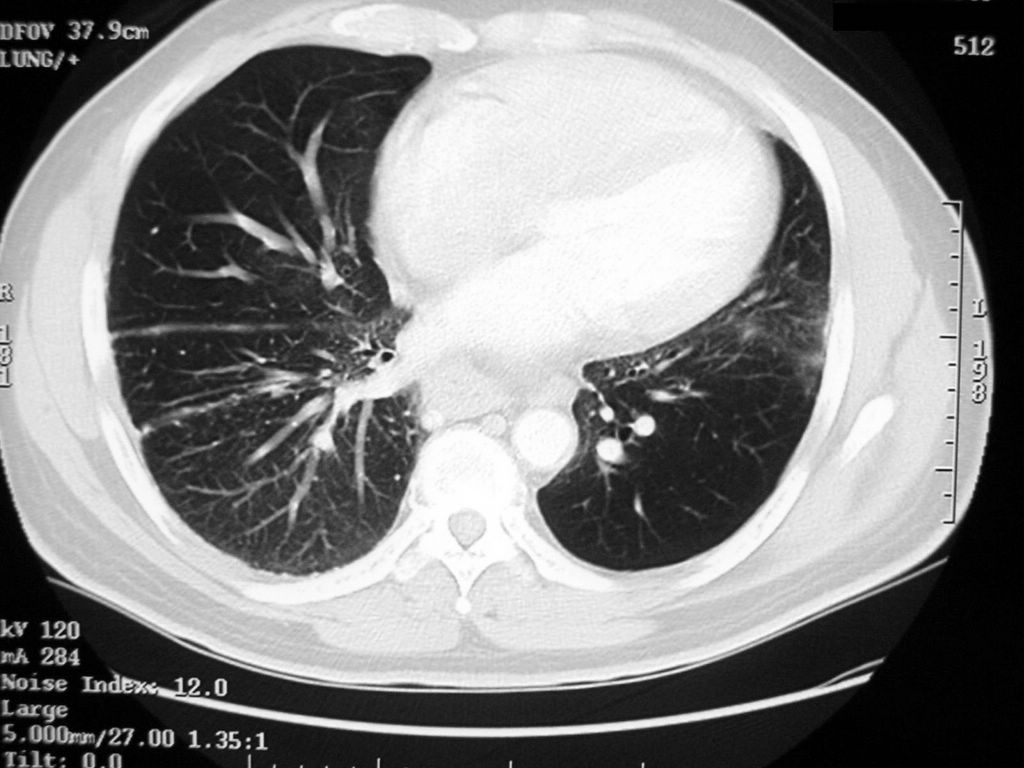
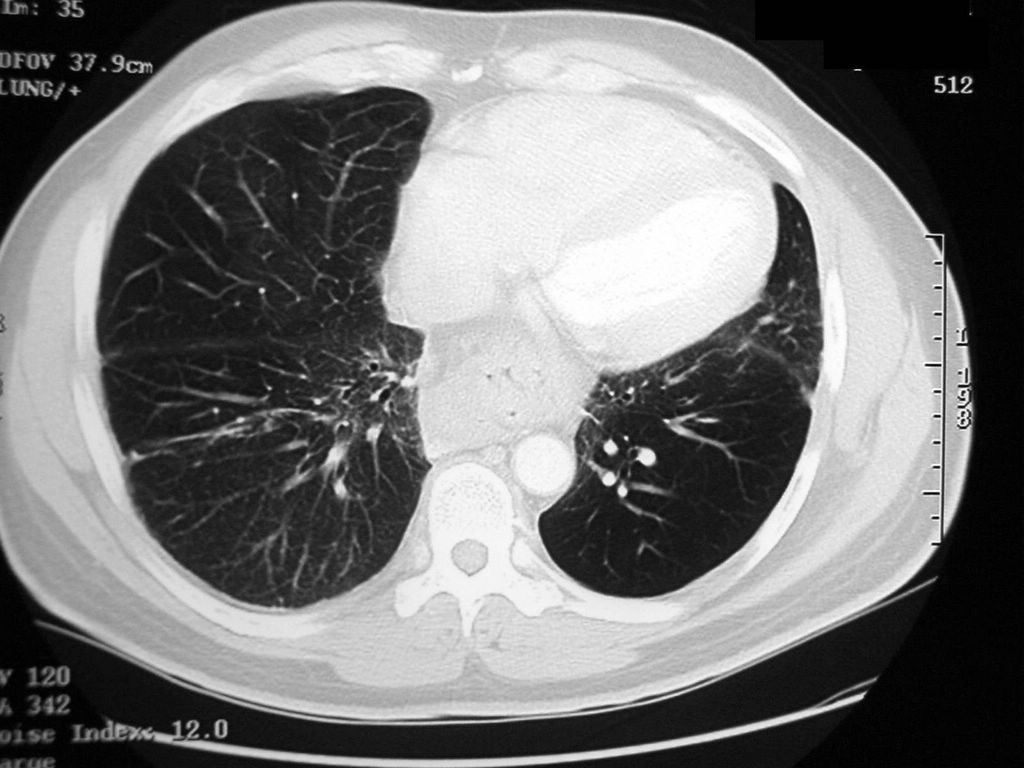
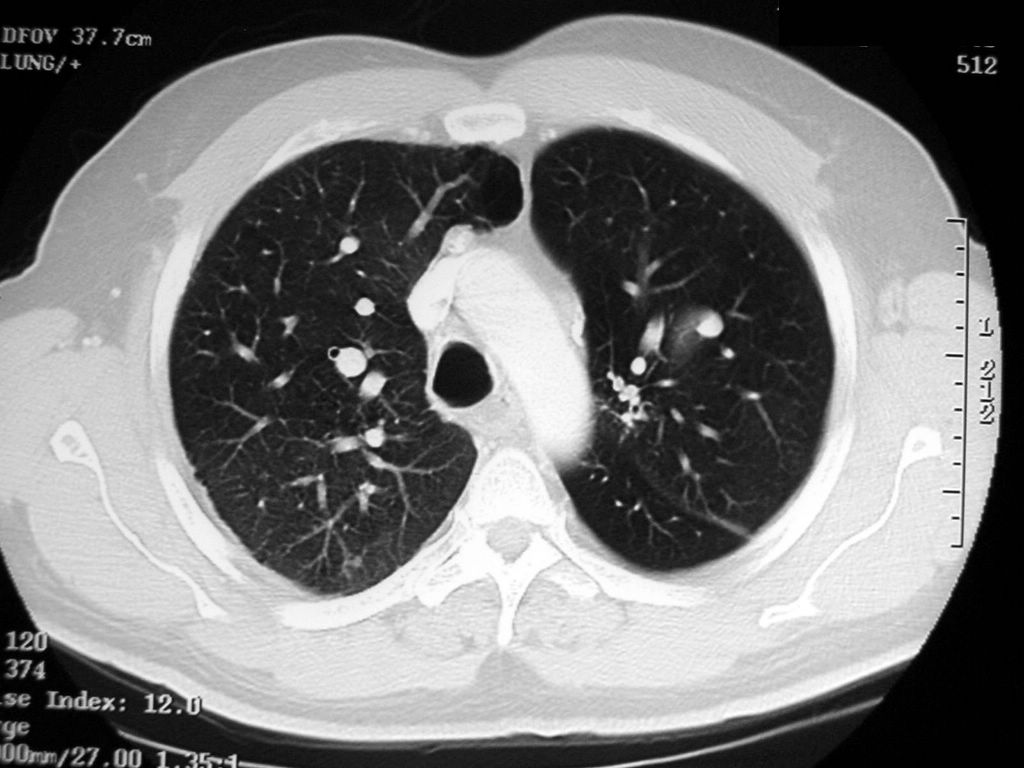
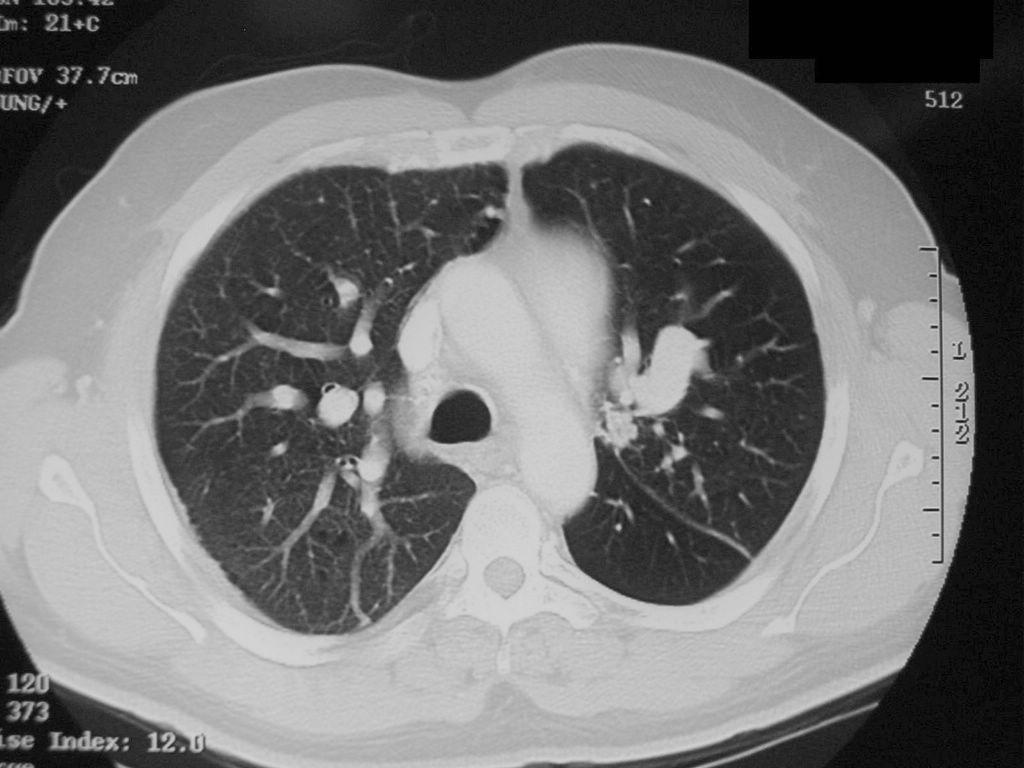
CT chest two years ago



CT chest two years ago
CT report:
Findings: There is a calcified left periaortic lymph node. Calcified mediastinal nodes are also noted. These findings are likely due to remote granulomatous. There is a large hiatal hernia.
Lung windows show COPD. Scarring is noted in the right lung base. Increased interstitial markings are seen in the medial right lung base possibly due to chronic change
There is infiltrate extending from the right hilum to the right lateral chest wall. Similar but less extensive infiltrate extends from the left hilum to the left lateral chest wall. Mild right hilar adenopathy is noted.
Impression:
1. Mild right hilar adenopathy with bilateral perihilar infiltrates right more extensive than left extending to the periphery.
2. Signs of remote granulomatous disease
3. Large hiatal hernia
4. Nonspecific left upper lobe nodule. Follow-up CT in four months is recommended to document stability
5. Increased interstitial markings in the lung bases especially medial right lung base. These could be chronic and possibly related to scarring.





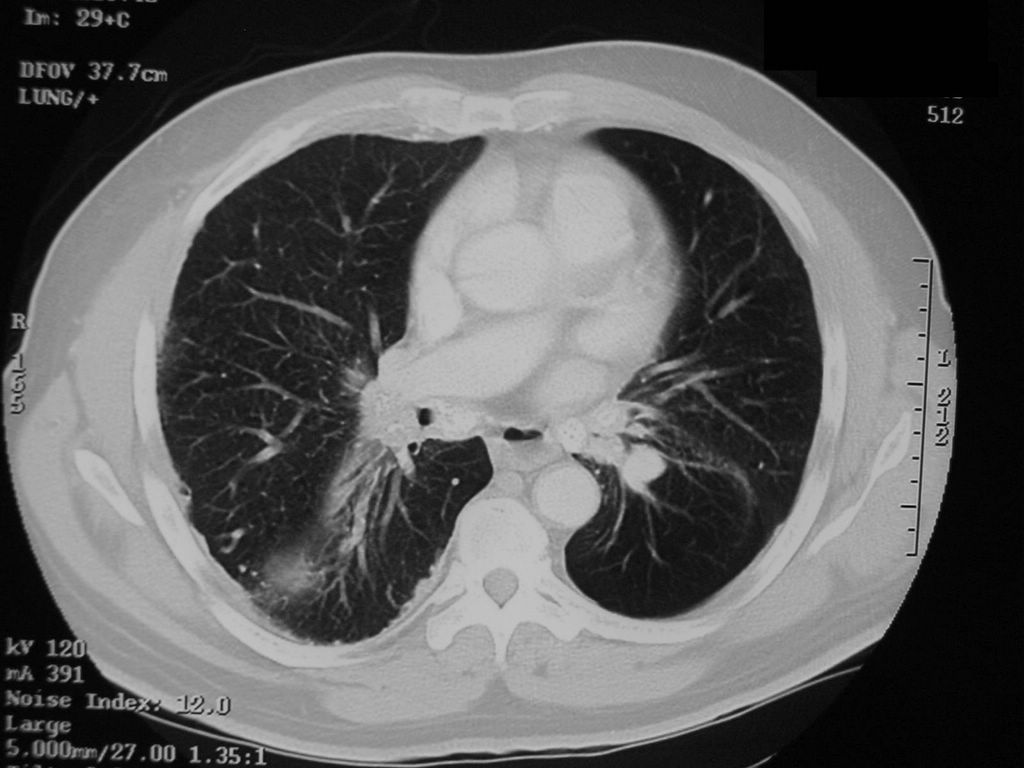
CT during this admission
CT chest report:
Since 2 years ago, again seen are enlarged mediastinal and hilar nodes some with calcifications. There is again a large hiatal hernia. There are enlarged bilateral pulmonary arteries creating the perihilar density seen on chest x-ray. Again seen are scars into both lung bases and infiltrates or atelectases/scars into the right middle and lower lobes. There is unchanged nonspecific ground glass parenchymal pattern in the left upper lobe. There is again diffuse haziness of the right lung. There are bilateral air cysts. There are bilateral upper lobe nodules which are stable. Again seen is bilateral pleural thickening right side greater than the left with fine nodular peripheral irregularity right side greater than the left.
Impression: Unchanged enlarged mediastinal and hilar nodes some with calcifications. New mildly enlarged retrocrural node.
Infiltrate, scar, atelectasis in the right middle and lower lobes with additional pulmonary parenchymal scars particularly in the lung bases. Unchanged mild pleural thickening which can be secondary to scar. Stable upper lobe nodules.
What did we miss when collecting the history?
Occupational exposure. Always ask about the former or current jobs when doing H&P for a patient with chronic lung disease.
As Osler said, in 80 percent of the time, the patient will give you the diagnosis if you ask the right questions. You may not even need the physical examination (but you always have to do it).
When asked what he worked before, this patient said he worked in a foundry for 3 years (occupational exposure to silica dust).
His previous computer records were reviewed carefully and he indeed had a lung biopsy. The problem was that the biopsy was not diagnostic for sarcoidosis. He had some of the features of the active disease, like elevated high ACE level but lacked some of the others like increased calcium.

Biopsy report
What happened?
He was started on Solu-Medrol 30 mg IV q 6 hr and aerosols q 4 hr. Gradually his symptoms resolved and he was discharged home. PPD was negative. The patient has a marked mediastinal lymphadenopathy which is not seen in pneumoconiosis and can be a feature of sarcoidosis. Lymphoma is is unlikely with such protracted disease course spanning several years. A second bronchoscopy with lymph node biopsy will be scheduled.
Final diagnosis: Pneumoconiosis and Suspected Sarcoidosis
What did we learn from this case?
Always collect occupational exposure history in patients with chronic lung disease. Do not be fooled by the "known history of" phrase because often when you look at the records, you will notice that the grounds for the particular diagnosis were not that firm.
What is a foundry?
An establishment where metal is melted and poured into molds. The molds are covered with sand from inside and then the heated metal is poured in. The sand evaporates from the heat and the air is filled with silica particles. After the metal cast cools of, its surface is still rough from the remaining silica particles and has to be smoothened. During this process there is even higher concentration of silica in the air.
All these occupational factors may lead to development of silicosis in foundry workers.
How are the pneumoconioses diagnosed?
By occupational history and CXR.
There is a classification for grading the severity of pneumoconioses - the PQRSTU system.
The PQRSTU System
The CXR shadow due to pneumoconioses are described as round or linear. The round shadows are graded in size from P (smallest) to R (largest). The linear shadows are graded from T (smallest) to U (largest).
This PQRSTU system reminds us of the PQRSTU nomenclature used to describe the different elements of the electrocardiogram.
PMH: Asthma/COPD, Sarcoidosis, HTN
Medications: Advair, inhalers, Lisinopril, HCTZ
SH: Former smoker
Physical examination:
VS 36.4-20-82-140/82
SpO2 98% on RA
Chest: decreased AE (B), wheezing (B)
CVS: Clear S1S2
Abdomen: Soft, NT, ND
Extremities: no c/c/e
What do you think is going on?
A typical asthma exacerbation?
Sarcoidosis flare-up?
Pneumonia?
Or something else?
What tests would you order?
CXR
CBCD, CMP
Sputum Gram stain, C+S
CXR
CXR two years ago. Close-up of the RLL.
CXR report: Since 2 years ago, limited portable upright view shows stable partially calcified hilar lymph nodes, pleural thickening of right minor fissure, the normal size heart. Previously demonstrated retrocardiac hiatus hernia is partly seen as a double density through the heart.

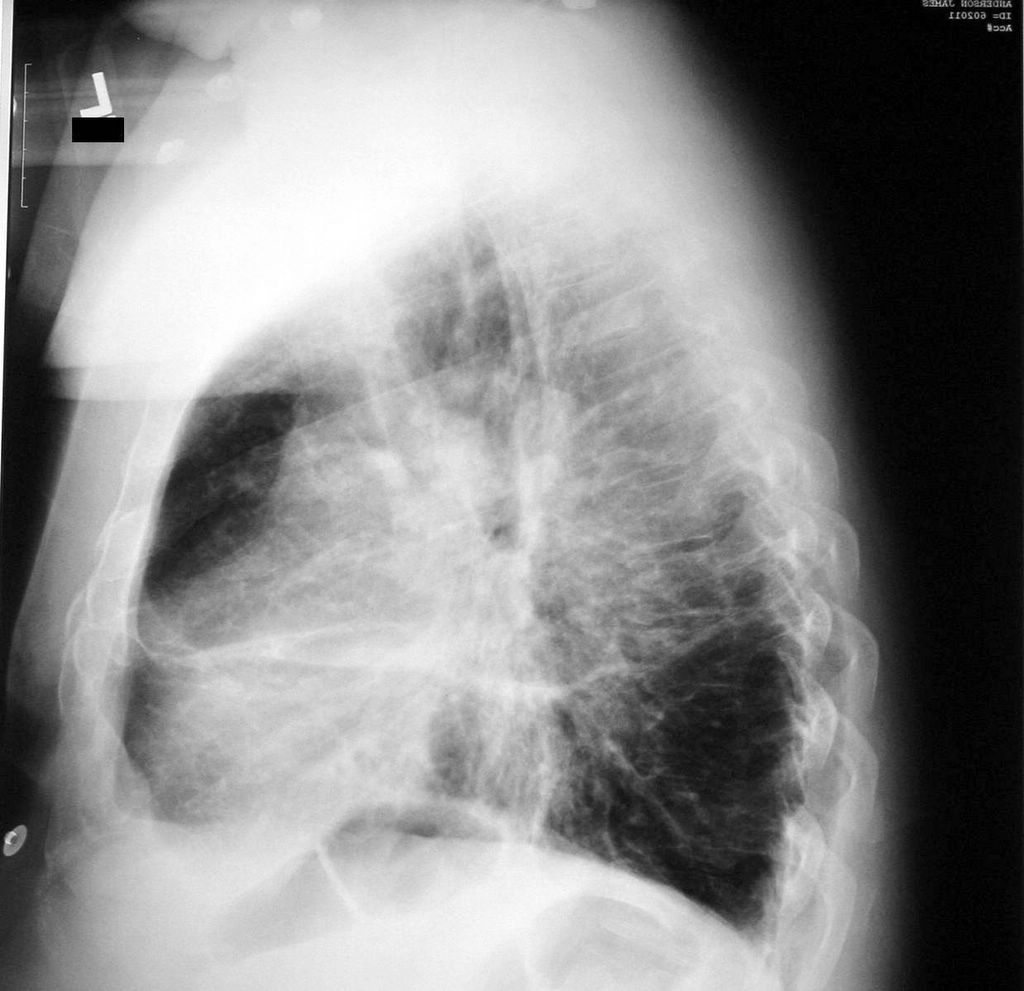

CXR on this admission; lateral CXR; report
He also had a CT scan of the chest which showed diffuse ground glass pattern.
CT chest two years ago

CT chest two years ago
CT report:
Findings: There is a calcified left periaortic lymph node. Calcified mediastinal nodes are also noted. These findings are likely due to remote granulomatous. There is a large hiatal hernia.
Lung windows show COPD. Scarring is noted in the right lung base. Increased interstitial markings are seen in the medial right lung base possibly due to chronic change
There is infiltrate extending from the right hilum to the right lateral chest wall. Similar but less extensive infiltrate extends from the left hilum to the left lateral chest wall. Mild right hilar adenopathy is noted.
Impression:
1. Mild right hilar adenopathy with bilateral perihilar infiltrates right more extensive than left extending to the periphery.
2. Signs of remote granulomatous disease
3. Large hiatal hernia
4. Nonspecific left upper lobe nodule. Follow-up CT in four months is recommended to document stability
5. Increased interstitial markings in the lung bases especially medial right lung base. These could be chronic and possibly related to scarring.

CT during this admission
CT chest report:
Since 2 years ago, again seen are enlarged mediastinal and hilar nodes some with calcifications. There is again a large hiatal hernia. There are enlarged bilateral pulmonary arteries creating the perihilar density seen on chest x-ray. Again seen are scars into both lung bases and infiltrates or atelectases/scars into the right middle and lower lobes. There is unchanged nonspecific ground glass parenchymal pattern in the left upper lobe. There is again diffuse haziness of the right lung. There are bilateral air cysts. There are bilateral upper lobe nodules which are stable. Again seen is bilateral pleural thickening right side greater than the left with fine nodular peripheral irregularity right side greater than the left.
Impression: Unchanged enlarged mediastinal and hilar nodes some with calcifications. New mildly enlarged retrocrural node.
Infiltrate, scar, atelectasis in the right middle and lower lobes with additional pulmonary parenchymal scars particularly in the lung bases. Unchanged mild pleural thickening which can be secondary to scar. Stable upper lobe nodules.
What did we miss when collecting the history?
Occupational exposure. Always ask about the former or current jobs when doing H&P for a patient with chronic lung disease.
As Osler said, in 80 percent of the time, the patient will give you the diagnosis if you ask the right questions. You may not even need the physical examination (but you always have to do it).
When asked what he worked before, this patient said he worked in a foundry for 3 years (occupational exposure to silica dust).
His previous computer records were reviewed carefully and he indeed had a lung biopsy. The problem was that the biopsy was not diagnostic for sarcoidosis. He had some of the features of the active disease, like elevated high ACE level but lacked some of the others like increased calcium.
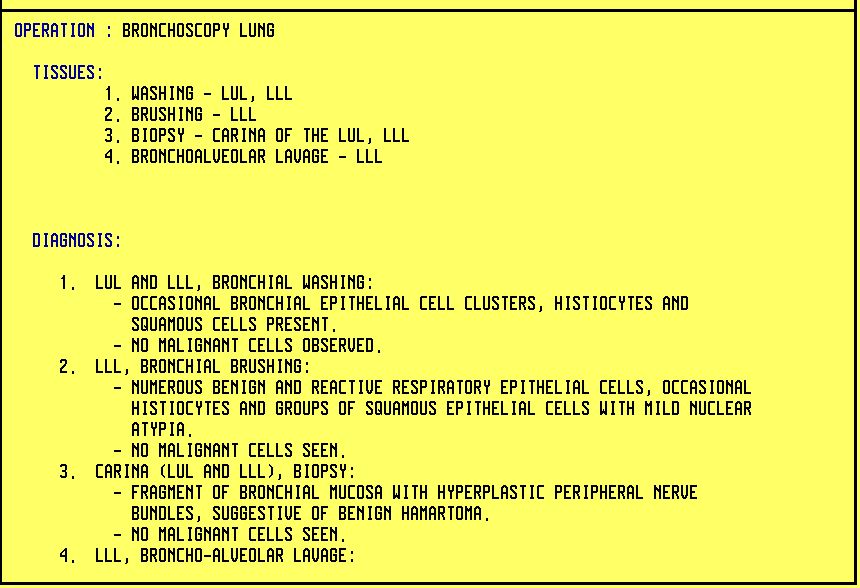
Biopsy report
What happened?
He was started on Solu-Medrol 30 mg IV q 6 hr and aerosols q 4 hr. Gradually his symptoms resolved and he was discharged home. PPD was negative. The patient has a marked mediastinal lymphadenopathy which is not seen in pneumoconiosis and can be a feature of sarcoidosis. Lymphoma is is unlikely with such protracted disease course spanning several years. A second bronchoscopy with lymph node biopsy will be scheduled.
Final diagnosis: Pneumoconiosis and Suspected Sarcoidosis
What did we learn from this case?
Always collect occupational exposure history in patients with chronic lung disease. Do not be fooled by the "known history of" phrase because often when you look at the records, you will notice that the grounds for the particular diagnosis were not that firm.
What is a foundry?
An establishment where metal is melted and poured into molds. The molds are covered with sand from inside and then the heated metal is poured in. The sand evaporates from the heat and the air is filled with silica particles. After the metal cast cools of, its surface is still rough from the remaining silica particles and has to be smoothened. During this process there is even higher concentration of silica in the air.
All these occupational factors may lead to development of silicosis in foundry workers.
How are the pneumoconioses diagnosed?
By occupational history and CXR.
There is a classification for grading the severity of pneumoconioses - the PQRSTU system.
The PQRSTU System
The CXR shadow due to pneumoconioses are described as round or linear. The round shadows are graded in size from P (smallest) to R (largest). The linear shadows are graded from T (smallest) to U (largest).
This PQRSTU system reminds us of the PQRSTU nomenclature used to describe the different elements of the electrocardiogram.