32 yo AAF was admitted to the hospital with aspiration pneumonia and respiratory failure. She was not weanable from the ventilator and a tracheostomy was placed. The patient was admitted to an acute long-term care facility where she was following a chronic weraning protocol. While there, she had had a cardiorespiratory arrest and developed anoxic encephalopathy. The family insists on full code.
She is in ICU on vent. ABGs and CXRs show ARDS. Serial CXRs revealed worsening right lung collapse.

ABGs in ARDS
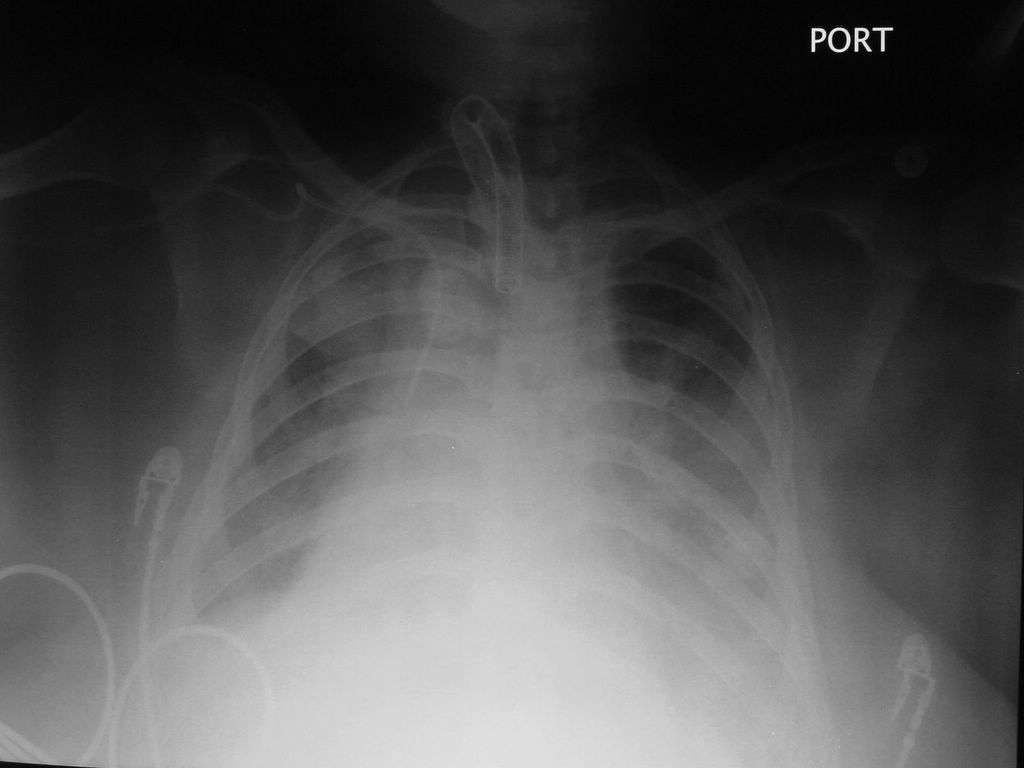
CXR


Right lung atelectasis with a shift of the mediastinum. ETT size 6 is too small to pass the bronschoscope for diagnosis and therapeutic suctioning.

Persistent atelectasis
CXR report:
Since yesterday, limited portable supine is the exam shows stable opaque right thorax mediastinal shift to the right, likely collapse of right lung with an endobronchial obstruction including underlying neoplasm considered as well as mucus plugging bronchogenic obstruction. Haziness of left mid and lower lung likely represents layering of left pleural effusion. Right cardiac border remains obscured.
What is the reason for the right lung opacification?
Mucus plug is the most likely cause for lung collapse in this patient.
DDx: CA (unlikely at this age)
What to do?
Bronchoscopy with mucus plug susctioning.
But first you have to check the size of the tracheostomy tube because the bronchoscope does not pass if the tube size is less than 8.
Her t-tube is 6. ENT consult was called and the t-tube was replaced with another one, size 8.
In the meantime, Mucomyst aerosol q 4 hr was started.
What happened?
Two hours after the t-tube was replaced and the tube was suctioned, the CXR showed a complete resolution of the right lung atelectasis. The oxygenation improved and the FiO2 was decreased. Mucomyst was stopped because it may act as an airway irritant on its own. A bronchoscopy was not needed.
CXR


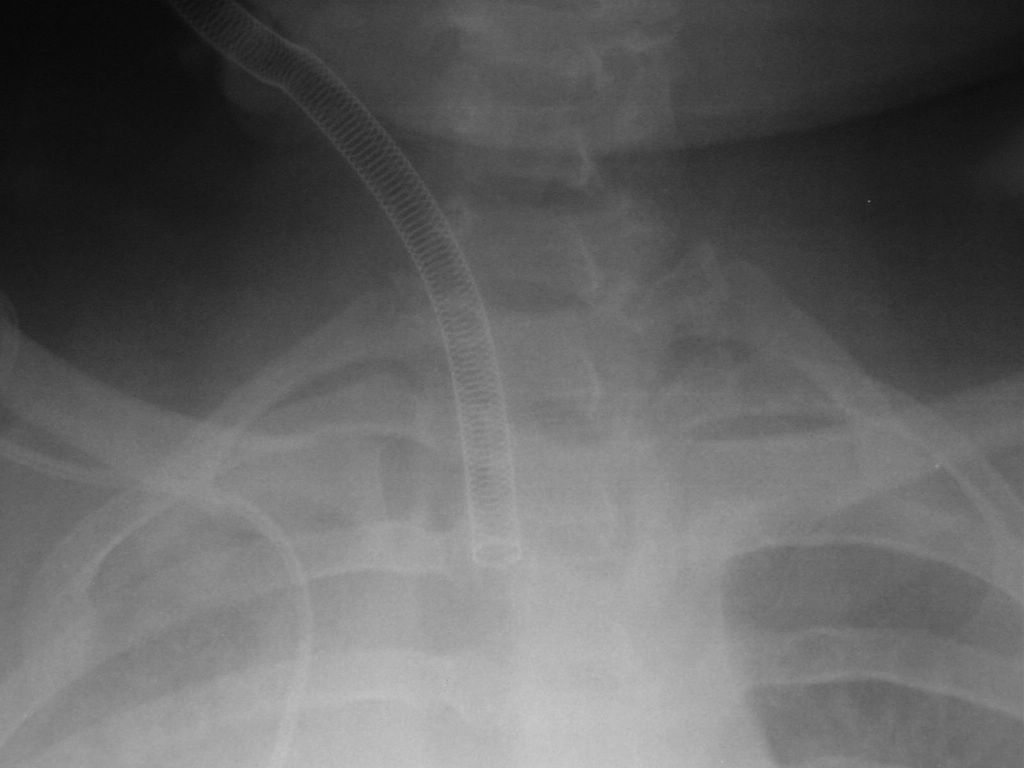
Trachea was suctioned and the ETT was changed with a larger one, size 8. The removed ETT was filled with thick yellow-grey mucus. The follow-up CXR showed reexpansion of the right lung. See the close-up of the ETT, size 8 is the minimal size allowing the passage of a bronchoscope.
CXR report:
There is improved aeration of the right lung. There are infiltrates or atelectases in the both lungs with pleural effusions. There is again cardiomegaly with pulmonary venous hypertension and CHF. The life support device placement is unchanged.

ABGs show a decrease in the required FiO2 after the atelectasis resolved
Final diagnosis: Right lung collapse in a ventilated patient due to mucus plug
What did we learn from this case?
There are several causes for sudden deterioration of oxygenation of a ventilated patient:
-Pneumothorax
-Atelectasis
-Pulmonary edema
Atelectasis is often due to mucus plug and can be resolved by suctioning of the ETT.
In all cases of sudden deterioration, the patient needs a CXR immediately.
She is in ICU on vent. ABGs and CXRs show ARDS. Serial CXRs revealed worsening right lung collapse.

ABGs in ARDS
CXR

Right lung atelectasis with a shift of the mediastinum. ETT size 6 is too small to pass the bronschoscope for diagnosis and therapeutic suctioning.

Persistent atelectasis
CXR report:
Since yesterday, limited portable supine is the exam shows stable opaque right thorax mediastinal shift to the right, likely collapse of right lung with an endobronchial obstruction including underlying neoplasm considered as well as mucus plugging bronchogenic obstruction. Haziness of left mid and lower lung likely represents layering of left pleural effusion. Right cardiac border remains obscured.
What is the reason for the right lung opacification?
Mucus plug is the most likely cause for lung collapse in this patient.
DDx: CA (unlikely at this age)
What to do?
Bronchoscopy with mucus plug susctioning.
But first you have to check the size of the tracheostomy tube because the bronchoscope does not pass if the tube size is less than 8.
Her t-tube is 6. ENT consult was called and the t-tube was replaced with another one, size 8.
In the meantime, Mucomyst aerosol q 4 hr was started.
What happened?
Two hours after the t-tube was replaced and the tube was suctioned, the CXR showed a complete resolution of the right lung atelectasis. The oxygenation improved and the FiO2 was decreased. Mucomyst was stopped because it may act as an airway irritant on its own. A bronchoscopy was not needed.
CXR

Trachea was suctioned and the ETT was changed with a larger one, size 8. The removed ETT was filled with thick yellow-grey mucus. The follow-up CXR showed reexpansion of the right lung. See the close-up of the ETT, size 8 is the minimal size allowing the passage of a bronchoscope.
CXR report:
There is improved aeration of the right lung. There are infiltrates or atelectases in the both lungs with pleural effusions. There is again cardiomegaly with pulmonary venous hypertension and CHF. The life support device placement is unchanged.
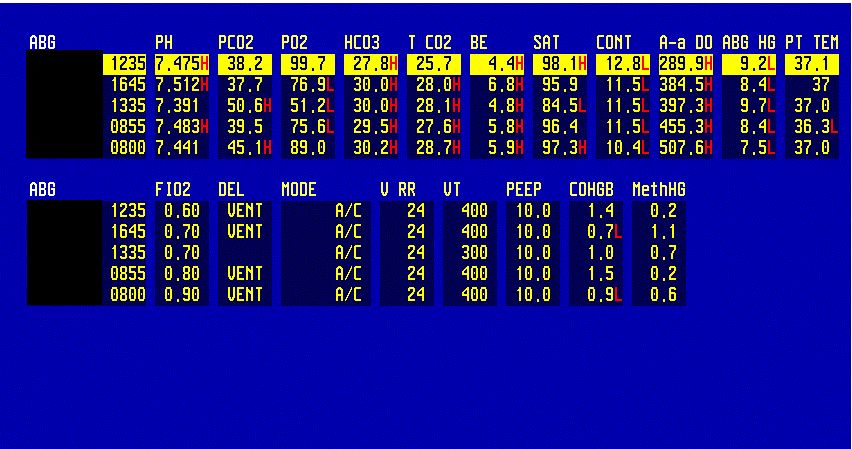
ABGs show a decrease in the required FiO2 after the atelectasis resolved
Final diagnosis: Right lung collapse in a ventilated patient due to mucus plug
What did we learn from this case?
There are several causes for sudden deterioration of oxygenation of a ventilated patient:
-Pneumothorax
-Atelectasis
-Pulmonary edema
Atelectasis is often due to mucus plug and can be resolved by suctioning of the ETT.
In all cases of sudden deterioration, the patient needs a CXR immediately.