70 yo AAM is admitted to the hospital with CC: generalized weakness and slurred speech for one day.
He denies any N/V/D/C, no CP, SOB, DOE, PND or cough, no headache. The patient is sleeping and dozing off, with slurred speech, and no other complaints of weakness at the time of admission. According to his wife, he started having slurred speech the morning of the admission, which was new for him.
PMH: HTN, DM 2, HCV, questionable CVA, CAD S/P catheterization 3 years ago, with a stent in RCA, Hypercholesterolemia, PVD, Pneumonia 5 months ago
PSH: Cholecystectomy and left leg surgery for MVA
Medications: Altace 10 mg po qd, Pletal 100 mg po bid, metformin 500 mg po bid, Lipitor 20 mg po qhs and aspirin 325 mg po qd
SH: Lives with his wife. Denies any alcohol. Smokes 1 ppd for 30 yrs
FMH: Denies any CVA or CAD
In the ER, the admitting doctor felt that the patient had slurred speech and some slight weakness of his left arm and left leg. He had a tremor in his right arm. Otherwise no other focal findings or meningeal signs were noticed. An aspirin was given. He was admitted with a suspected stroke.
Physical exam on the ward:
WD/WN in NAD, very lethargic
VS: 36.4-20-129/60-67
Chest: CTA (B)
CVS: Clear S1S2, RRR
Abdomen: Soft, NT, ND, +BS
Ext: no c/c/e
Neuro exam:
Mental status: lethargic but arousable with dysarthria. He is oriented to "hospital," but not to the year or month. The patient, when awake, is slightly paranoid and wonders why we are there. He is frequently drowsy, dropping off to sleep in the midst of the exam, limiting it.
When he is asked who he is, he states he is named "Walker Smith" and he was born 20 years ago. We discussed this with his wife and she does not know anyone named Walker Smith.
Non-focal exam:
CN: Pupils are responsive bilaterally. EOM movements are present. There is no facial asymmetry. The patient can protrude his tongue to command without deviation.
The patient has antigravity power in all four extremities. Focal motor testing is difficult because of the patient's drowsiness, but his movements appear symmetric.
Sensory examination is intact to nail bed pressure throughout as the patient withdraws each of his limbs, symmetrically.
Muscle stretch reflexes are absent at the ankles, present at the knees, and normal in the arms. The plantar responses are flexor.
Finger-to-nose and heel-to-shin testing are normal. Gait could not be evaluated because of the patient's drowsiness.
He has a non-focal neurological examination and clinically has no evidence for an acute stroke.
It would be interesting to know what his cognitive status was prior to this hospitalization.
What do you think is going on?
Change in mental status - this is clear but what is the reason?
Any of the 3 Ds: Delirium? Dementia? Depression?
/\MS DDx can be remembered by using the mnemonic ITS COMA:
Infection
Trauma, e.g. leading to subdural hemorrhage
Seizure
CO poisoning
Overdose
Metabolic abnormalities, e.g hyperNa+, DKA
Alcohol
What labs would you order?
CBCD, CMP, UA
CPP x 2 q 8 hr
EKG, CXR
CT of the head w/o contrast
Labs:
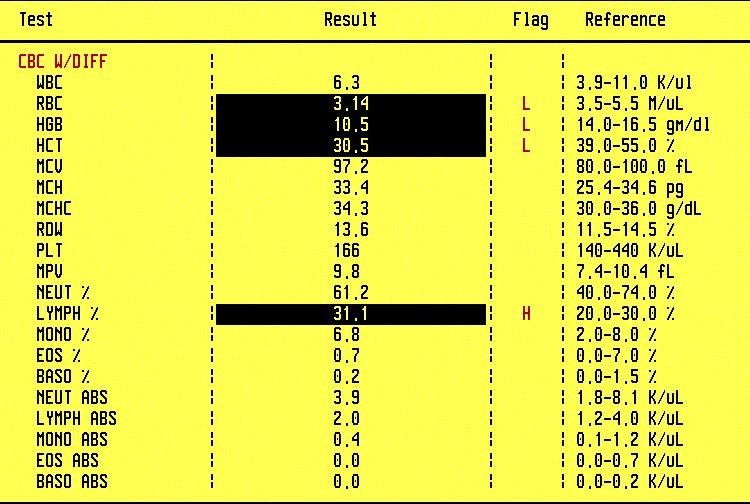
WBC 6.3, Hgb 10.5
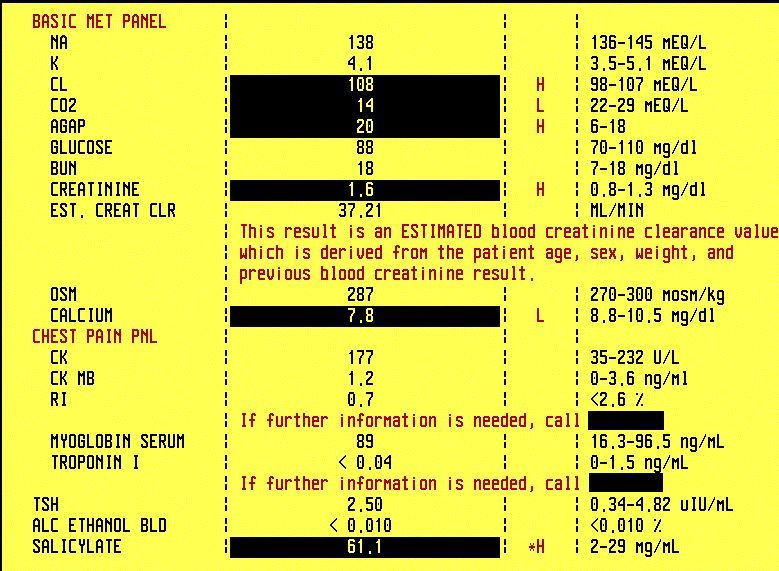
Anion gap is 16
Chest pain panels are negative


CBCD; CMP shows metabolic acidosis
Noncontrast cranial CT: extensive periventricular white matter disease, focal hypodensity in the left thalamus represents ischemia of undetermined age, remote infarct in the right side of the pons, no hemorrhage, moderate atrophy.
The EKG shows NSR, CXR is unremarkable.
ABG: pH 7.44, PaCO2 21, PaO2 101, HCO3 14 on RA

Urinalysis with toxic screen is positive for ketones
What happened?
Initially, patient was admitted to the regular floor with a preliminary diagnosis of stroke. But the neuro exam was non-focal and there is no clear evidence of acute event on CT of the head. The neurologist confirmed the diagnosis of metabolic encephalopathy and ruled out stroke.
What is the reason for the high AG metabolic acidosis?
The DDx list can be remembered by the now classic mnemonic MUD PILES or as Dr. Tahir says "when somebody is having high AG metabolic acidosis, your job is easy, because there only so many causes for it, and you just tick them off the list one by one".
MUD PILES:
Methanol - negative
Uremia - he has Cr 1.6 which can be due to dehydration or more likely to the ketones. He is not uremic with BUN of just 20.
DKA - he has ketones in the urine due to the fact that he missed some meals but he is not in DKA
Paraldehyde
INH or Iron
Lactate - he takes Metformin and Cr is 1.6 but his lactic acid level is normal
Ethylene glycol - negative
Salicylates - let's order a level...
What happened next?
In the work-up of metabolic acidosis, a salicylate level was ordered and patient was transferred to ICU because of increasing lethargy and worsening acidosis.


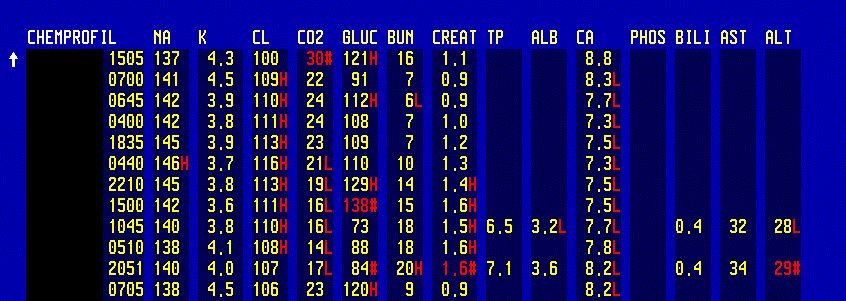
BMP and Salicylate level on admission; BMP done 4 days later shows acidosis resolution
Salicylate level was 61 (normal 2-29). The patient had his urine alkalinized with two amps of HCO3, and then a bicarb drip with potassium 20 mEq in D5W which helped eliminate the salicylate. The patient's electrolytes and pH were both monitored and the urine pH was kept above 7.5 to help excrete the salicylates.


ABG in salicylate toxicity; Serial ABGs should be done Q 2 hr (same as ASA levels and urine pH) to prevent severe alkalemia (arterial pH >7.60)
The patient's mental status gradually began to improve and the salicylate level was decreasing. Once the patient's mental status improved, he did state that he takes chronically 5-6 aspirins per day, maybe even more. The patient does not know why he is taking it. He does not admit any joint pain or any other pain. The patient was discharged to a rehabilation unit in good condition.

Salicylate levels - note that the patient had two episodes of salicylate toxicity, the second one was several months after this admission. Levels should be checked Q 2 hr until two consecutive levels show a decline.
Final diagnosis: Encephalopathy due to salicylate intoxication
What did we learn from this case?
Do not assume that the admitting diagnosis is right. In this case the slurred speech was not due to stroke but to salicylate toxicity.
Common things happen commonly but you have to go over the complete list of differentials, in this case MUD PILES, to be sure that you do not miss something important.
In ASA toxicity, monitor 3 levels Q 2 hr until improvement - salicylate level, pH, ABG.
The mainstay of therapy is bicarbonate IV and the goal is simple - alkalinize serum and urine. The logic behind the bicarbonate treatment is in the formula below:
H+ + ASA- < — > H-ASA
H-ASA easily moves across BBB and the renal tubules
Metabolic acidosis drives the reaction to the right and increases H-ASA, promoting diffusion across BBB into CNS.
Bicarb lowers H+ ion concentration and drives the above reaction to the left. ASA anions are "trapped" in the blood in a charged form and do not diffuse across BBB.
References:
Salicylate Toxicity - eMedicine (free)
Management of aspirin intoxication - UpToDate (paid subscription required)
He denies any N/V/D/C, no CP, SOB, DOE, PND or cough, no headache. The patient is sleeping and dozing off, with slurred speech, and no other complaints of weakness at the time of admission. According to his wife, he started having slurred speech the morning of the admission, which was new for him.
PMH: HTN, DM 2, HCV, questionable CVA, CAD S/P catheterization 3 years ago, with a stent in RCA, Hypercholesterolemia, PVD, Pneumonia 5 months ago
PSH: Cholecystectomy and left leg surgery for MVA
Medications: Altace 10 mg po qd, Pletal 100 mg po bid, metformin 500 mg po bid, Lipitor 20 mg po qhs and aspirin 325 mg po qd
SH: Lives with his wife. Denies any alcohol. Smokes 1 ppd for 30 yrs
FMH: Denies any CVA or CAD
In the ER, the admitting doctor felt that the patient had slurred speech and some slight weakness of his left arm and left leg. He had a tremor in his right arm. Otherwise no other focal findings or meningeal signs were noticed. An aspirin was given. He was admitted with a suspected stroke.
Physical exam on the ward:
WD/WN in NAD, very lethargic
VS: 36.4-20-129/60-67
Chest: CTA (B)
CVS: Clear S1S2, RRR
Abdomen: Soft, NT, ND, +BS
Ext: no c/c/e
Neuro exam:
Mental status: lethargic but arousable with dysarthria. He is oriented to "hospital," but not to the year or month. The patient, when awake, is slightly paranoid and wonders why we are there. He is frequently drowsy, dropping off to sleep in the midst of the exam, limiting it.
When he is asked who he is, he states he is named "Walker Smith" and he was born 20 years ago. We discussed this with his wife and she does not know anyone named Walker Smith.
Non-focal exam:
CN: Pupils are responsive bilaterally. EOM movements are present. There is no facial asymmetry. The patient can protrude his tongue to command without deviation.
The patient has antigravity power in all four extremities. Focal motor testing is difficult because of the patient's drowsiness, but his movements appear symmetric.
Sensory examination is intact to nail bed pressure throughout as the patient withdraws each of his limbs, symmetrically.
Muscle stretch reflexes are absent at the ankles, present at the knees, and normal in the arms. The plantar responses are flexor.
Finger-to-nose and heel-to-shin testing are normal. Gait could not be evaluated because of the patient's drowsiness.
He has a non-focal neurological examination and clinically has no evidence for an acute stroke.
It would be interesting to know what his cognitive status was prior to this hospitalization.
What do you think is going on?
Change in mental status - this is clear but what is the reason?
Any of the 3 Ds: Delirium? Dementia? Depression?
/\MS DDx can be remembered by using the mnemonic ITS COMA:
Infection
Trauma, e.g. leading to subdural hemorrhage
Seizure
CO poisoning
Overdose
Metabolic abnormalities, e.g hyperNa+, DKA
Alcohol
What labs would you order?
CBCD, CMP, UA
CPP x 2 q 8 hr
EKG, CXR
CT of the head w/o contrast
Labs:
WBC 6.3, Hgb 10.5
Anion gap is 16
Chest pain panels are negative
CBCD; CMP shows metabolic acidosis
Noncontrast cranial CT: extensive periventricular white matter disease, focal hypodensity in the left thalamus represents ischemia of undetermined age, remote infarct in the right side of the pons, no hemorrhage, moderate atrophy.
The EKG shows NSR, CXR is unremarkable.
ABG: pH 7.44, PaCO2 21, PaO2 101, HCO3 14 on RA
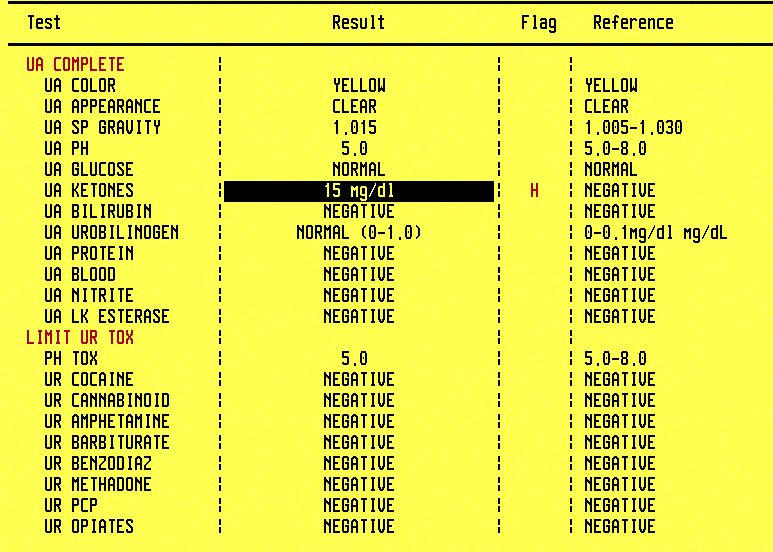
Urinalysis with toxic screen is positive for ketones
What happened?
Initially, patient was admitted to the regular floor with a preliminary diagnosis of stroke. But the neuro exam was non-focal and there is no clear evidence of acute event on CT of the head. The neurologist confirmed the diagnosis of metabolic encephalopathy and ruled out stroke.
What is the reason for the high AG metabolic acidosis?
The DDx list can be remembered by the now classic mnemonic MUD PILES or as Dr. Tahir says "when somebody is having high AG metabolic acidosis, your job is easy, because there only so many causes for it, and you just tick them off the list one by one".
MUD PILES:
Methanol - negative
Uremia - he has Cr 1.6 which can be due to dehydration or more likely to the ketones. He is not uremic with BUN of just 20.
DKA - he has ketones in the urine due to the fact that he missed some meals but he is not in DKA
Paraldehyde
INH or Iron
Lactate - he takes Metformin and Cr is 1.6 but his lactic acid level is normal
Ethylene glycol - negative
Salicylates - let's order a level...
What happened next?
In the work-up of metabolic acidosis, a salicylate level was ordered and patient was transferred to ICU because of increasing lethargy and worsening acidosis.
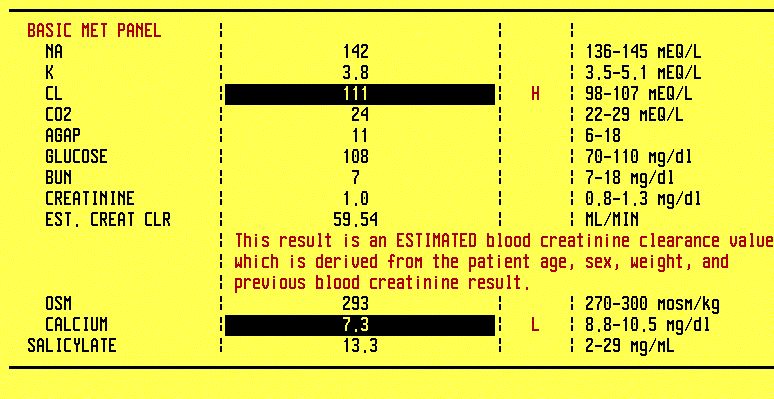
BMP and Salicylate level on admission; BMP done 4 days later shows acidosis resolution
Salicylate level was 61 (normal 2-29). The patient had his urine alkalinized with two amps of HCO3, and then a bicarb drip with potassium 20 mEq in D5W which helped eliminate the salicylate. The patient's electrolytes and pH were both monitored and the urine pH was kept above 7.5 to help excrete the salicylates.
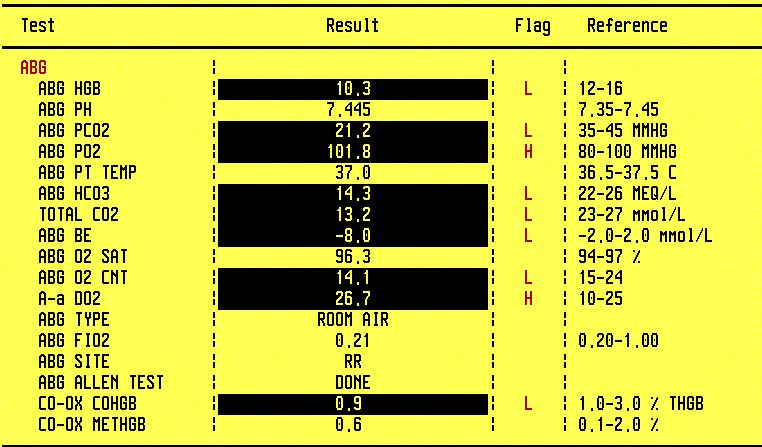
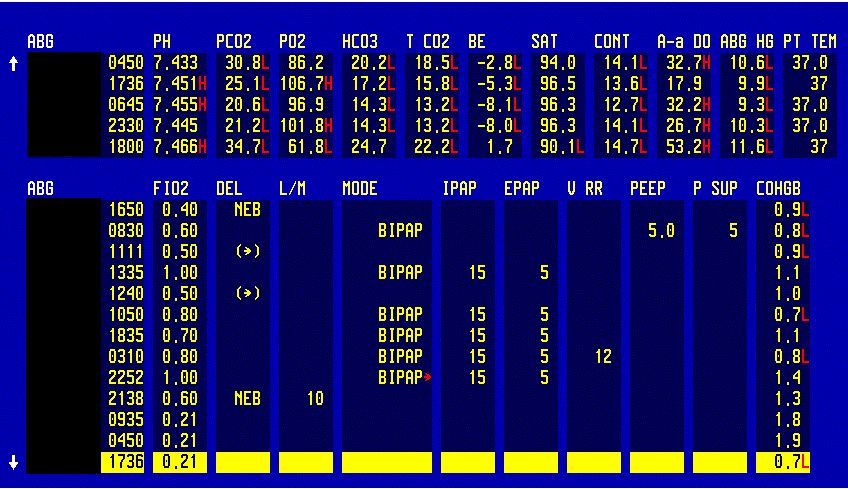
ABG in salicylate toxicity; Serial ABGs should be done Q 2 hr (same as ASA levels and urine pH) to prevent severe alkalemia (arterial pH >7.60)
The patient's mental status gradually began to improve and the salicylate level was decreasing. Once the patient's mental status improved, he did state that he takes chronically 5-6 aspirins per day, maybe even more. The patient does not know why he is taking it. He does not admit any joint pain or any other pain. The patient was discharged to a rehabilation unit in good condition.

Salicylate levels - note that the patient had two episodes of salicylate toxicity, the second one was several months after this admission. Levels should be checked Q 2 hr until two consecutive levels show a decline.
Final diagnosis: Encephalopathy due to salicylate intoxication
What did we learn from this case?
Do not assume that the admitting diagnosis is right. In this case the slurred speech was not due to stroke but to salicylate toxicity.
Common things happen commonly but you have to go over the complete list of differentials, in this case MUD PILES, to be sure that you do not miss something important.
In ASA toxicity, monitor 3 levels Q 2 hr until improvement - salicylate level, pH, ABG.
The mainstay of therapy is bicarbonate IV and the goal is simple - alkalinize serum and urine. The logic behind the bicarbonate treatment is in the formula below:
H+ + ASA- < — > H-ASA
H-ASA easily moves across BBB and the renal tubules
Metabolic acidosis drives the reaction to the right and increases H-ASA, promoting diffusion across BBB into CNS.
Bicarb lowers H+ ion concentration and drives the above reaction to the left. ASA anions are "trapped" in the blood in a charged form and do not diffuse across BBB.
References:
Salicylate Toxicity - eMedicine (free)
Management of aspirin intoxication - UpToDate (paid subscription required)