58 yo AAM was admitted from a NH with CC: lethargic and not acting appropriately. The patient stated that his legs hurt, and they had been hurting for a long time.
PMH: DM, HTN, venous stasis ulcers, Anemia, hepatitis C, PVD, CHF
PSH: (B) LE stasis ulcers S/P debridement and multiple failed skin grafts 2 years ago, right hallux amputation
Medications: Tylenol, Ambien, hydrocodone, FeSO4, clonidine, amitriptyline, Oxycontin, Lantus, Lasix, metformin, Actos, metoprolol
SH: remote history of heroin and cocaine abuse, former smoker and drinker
Physical exam:
VS 38-126-24-137/81
Chest: CTA (B)
CVS: tachycardic but regular with no murmurs
Abdomen: Soft, NT, ND, +BS
Extremities: severe venous stasis ulcers of the lower extremities (B)
Neuro: AAO x 2. No focal neurological deficits apart from diminished sensation on (B) LE.

Diabetic patient with (B) infected stasis ulcers
What labs would you order?
CBCD, CMP, UA
Wound culture, BC x 2
X-rays



CBC in IDA, CMP, the hypogycemia was corrected; CBCD; Iron profile and prealbumin.
Iron and iron saturation are low but the ferritin is high and the TIBC is low. What is the reason?
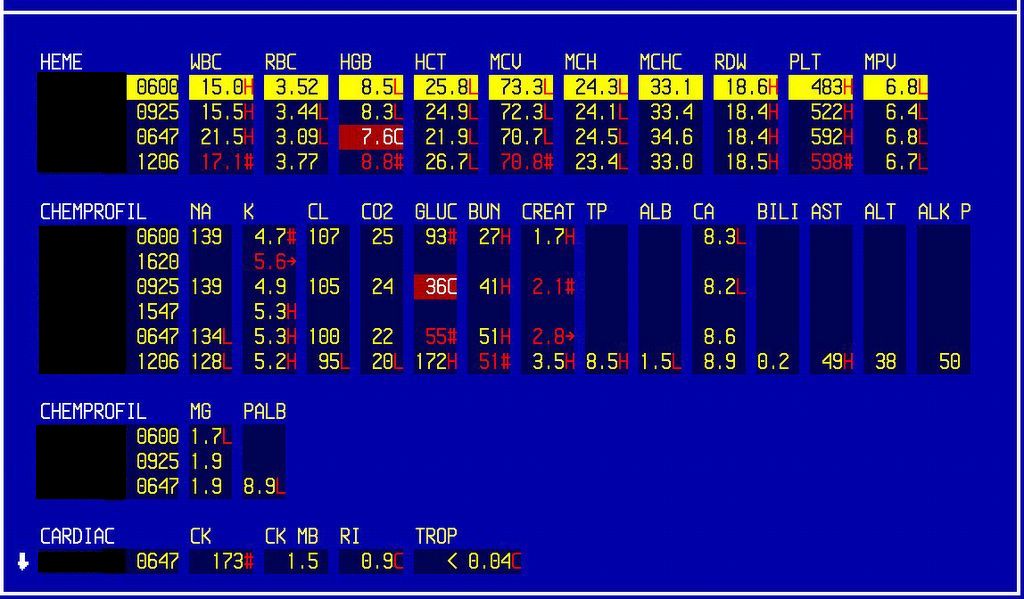
BUN was 51 and creatinine 2.5
Hgb 8.8
What are the questions to ask now?
What is his baseline?
A review of the old medical records, showed a BUN of 14 and creatinine of 1.3, seven months ago.
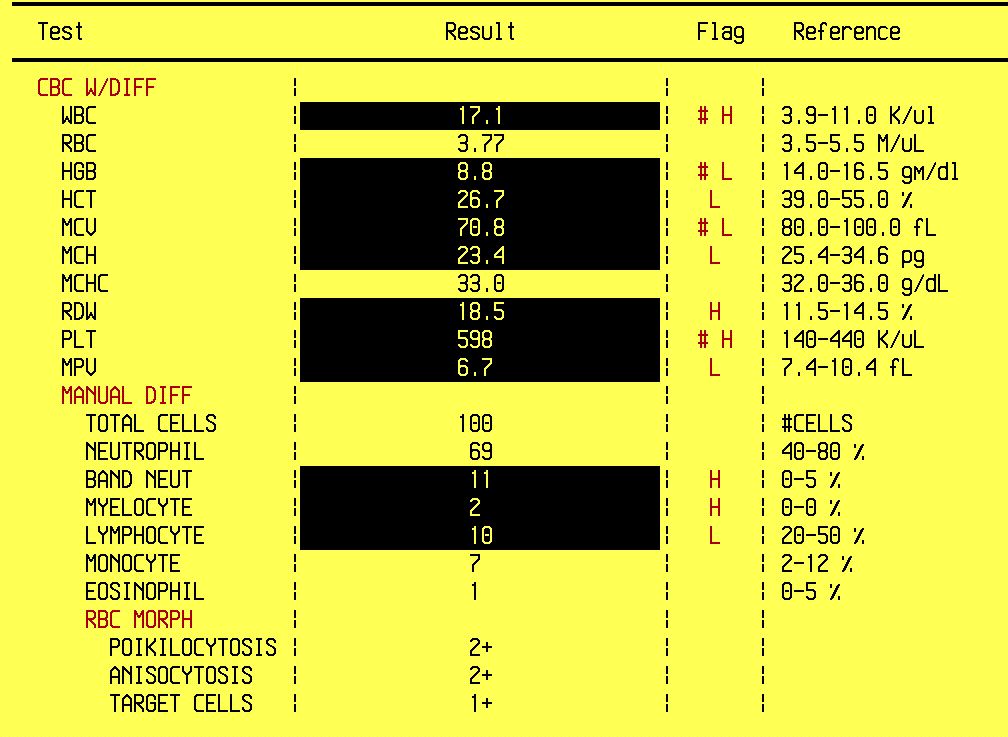
WBC was 17.1, hemoglobin 8.8, hematocrit 26.7, hypochromic, microcytic peripheral smear. The differential showed 69 neutrophils and 11 bands.
The patient has an infection, and he is probably dehydrated which may explain the rise in the BUN/Cr. Mucosal membranes are dry.
What happened?
Patient was admitted to telemetry. Zosyn and IV fluids were given.
The following day, patient's hemoglobin dropped to 7.6.
What do you think is the reason?
Mainly hemodilution - check the input and ouput summary over the last 24 hours (I/O). He was 3 L positive.
I/O showed that the patient was 3 liters positive
The patient was transfused 2 U PRBC, iron profile and ferritin were ordered as add-on tests.
The iron profile showed severe iron deficiency bu why the ferritin is high?
The patient is having wound infection and this is the reason for the high ferritin and platelets.
TIBC is low because he also has anemia of chronic disease.
Note how the BUN and Cr returned to baseline values with rehydration.
What is the reason for the iron deficiency anemia? Is he bleeding?
You are right - this is the most urgent question - is the patient bleeding?
How can we decide?
He is hemodynamically stable, i.e. VSS, no orthostatic changes
Rectal exam showed brown stool, negative for occult blood
H/H is stable
There are several reasons for iron derficiency anemia, remembered by the mnemonic NIMBLE:
Need - increased need as in pregnancy, children during stages of rapid growth
Intake is low, e.g. in malnutriton
Malabsorption
Blood
Loss, e.g. GI bleeding
Excessive donation, e.g. in blood donors
What happened to this patient?
Prealbumin was very low - 9.2. The most likely reason for the iron deficiency anemia is malnutriton due to poor PO intake.
He received 2 U PRBC. Blood conservation protocol was started with Iron and Epogen.
Nutrition consult was called.
Final diagnosis: Iron deficiency anemia (IDA) secondary to malnutrtion. Anemia of chronic disease due to CRI.
What did we learn from this case?
The most dangerous cause for IDA is GI bleeding and it needs to be ruled out first.
Consider poor PO intake in the differential especially in the debilitated patients with miltiple comorbidies.
A drop in the hemoglobin can be due to hemodilution. This is especially true in dehydrated patients with preexistent anemia. The rule of thumb is one liter of IVF drops the Hgb by one gm/dL.
Use the blood conservation protocol early. Giving blood has the disadvantages of being expensive and exposing patients to infections.
Resources:
Epogen / Iron Protocol for General Medical and General Surgical Patients
Indications for Use
Bone marrow stimulant for those who refuse blood and/or have had a significant acute blood loss without co-morbidities or Hgb <9.0 gm/dl with comorbidities. Use in patients who would benefit from accelerated red cell production in order to reduce the need for blood transfusion. Note: Guidelines are not for renal dosing or some hematological problems.
Step 1: Consider assessing for:
Iron deficiency, infection, inflammation, blood loss, malignancy, hematological problems, B9 and 12 vitamin deficiency, malabsorption, chronic renal insufficiency or failure.
Step 2: Baseline Lab studies:
CBC, reticulocyte count, iron panel
Step 3: Ensure adequate iron stores:
Iron saturation <30%:
____ Iron Sucrose 100 mg IV once a day x________________(total maximum dose 1000 mg or 10 doses )
Or
____ Iron Sucrose 300 mg IV every other day for three (3) doses
Step 4: Oral medications:
Folic Acid 1 mg PO QD
Vitamin C 500 mg PO QD
Vitamin B12 1000 mcg IM x 1 dose
Step 5: Epogen:
____ 20,000 units SQ three (3) times a week until hemoglobin >/= 10 gm/dl
____ Bloodless patient hemoglobin <5>/= 10 gm/dl
Step 6: Monitor and evaluate:
____ CBC, reticulocyte count 7 days from initiation of treatment
PMH: DM, HTN, venous stasis ulcers, Anemia, hepatitis C, PVD, CHF
PSH: (B) LE stasis ulcers S/P debridement and multiple failed skin grafts 2 years ago, right hallux amputation
Medications: Tylenol, Ambien, hydrocodone, FeSO4, clonidine, amitriptyline, Oxycontin, Lantus, Lasix, metformin, Actos, metoprolol
SH: remote history of heroin and cocaine abuse, former smoker and drinker
Physical exam:
VS 38-126-24-137/81
Chest: CTA (B)
CVS: tachycardic but regular with no murmurs
Abdomen: Soft, NT, ND, +BS
Extremities: severe venous stasis ulcers of the lower extremities (B)
Neuro: AAO x 2. No focal neurological deficits apart from diminished sensation on (B) LE.

Diabetic patient with (B) infected stasis ulcers
What labs would you order?
CBCD, CMP, UA
Wound culture, BC x 2
X-rays

CBC in IDA, CMP, the hypogycemia was corrected; CBCD; Iron profile and prealbumin.
Iron and iron saturation are low but the ferritin is high and the TIBC is low. What is the reason?
BUN was 51 and creatinine 2.5
Hgb 8.8
What are the questions to ask now?
What is his baseline?
A review of the old medical records, showed a BUN of 14 and creatinine of 1.3, seven months ago.
WBC was 17.1, hemoglobin 8.8, hematocrit 26.7, hypochromic, microcytic peripheral smear. The differential showed 69 neutrophils and 11 bands.
The patient has an infection, and he is probably dehydrated which may explain the rise in the BUN/Cr. Mucosal membranes are dry.
What happened?
Patient was admitted to telemetry. Zosyn and IV fluids were given.
The following day, patient's hemoglobin dropped to 7.6.
What do you think is the reason?
Mainly hemodilution - check the input and ouput summary over the last 24 hours (I/O). He was 3 L positive.

I/O showed that the patient was 3 liters positive
The patient was transfused 2 U PRBC, iron profile and ferritin were ordered as add-on tests.
The iron profile showed severe iron deficiency bu why the ferritin is high?
The patient is having wound infection and this is the reason for the high ferritin and platelets.
TIBC is low because he also has anemia of chronic disease.
Note how the BUN and Cr returned to baseline values with rehydration.
What is the reason for the iron deficiency anemia? Is he bleeding?
You are right - this is the most urgent question - is the patient bleeding?
How can we decide?
He is hemodynamically stable, i.e. VSS, no orthostatic changes
Rectal exam showed brown stool, negative for occult blood
H/H is stable
There are several reasons for iron derficiency anemia, remembered by the mnemonic NIMBLE:
Need - increased need as in pregnancy, children during stages of rapid growth
Intake is low, e.g. in malnutriton
Malabsorption
Blood
Loss, e.g. GI bleeding
Excessive donation, e.g. in blood donors
What happened to this patient?
Prealbumin was very low - 9.2. The most likely reason for the iron deficiency anemia is malnutriton due to poor PO intake.
He received 2 U PRBC. Blood conservation protocol was started with Iron and Epogen.
Nutrition consult was called.
Final diagnosis: Iron deficiency anemia (IDA) secondary to malnutrtion. Anemia of chronic disease due to CRI.
What did we learn from this case?
The most dangerous cause for IDA is GI bleeding and it needs to be ruled out first.
Consider poor PO intake in the differential especially in the debilitated patients with miltiple comorbidies.
A drop in the hemoglobin can be due to hemodilution. This is especially true in dehydrated patients with preexistent anemia. The rule of thumb is one liter of IVF drops the Hgb by one gm/dL.
Use the blood conservation protocol early. Giving blood has the disadvantages of being expensive and exposing patients to infections.
Resources:
Epogen / Iron Protocol for General Medical and General Surgical Patients
Indications for Use
Bone marrow stimulant for those who refuse blood and/or have had a significant acute blood loss without co-morbidities or Hgb <9.0 gm/dl with comorbidities. Use in patients who would benefit from accelerated red cell production in order to reduce the need for blood transfusion. Note: Guidelines are not for renal dosing or some hematological problems.
Step 1: Consider assessing for:
Iron deficiency, infection, inflammation, blood loss, malignancy, hematological problems, B9 and 12 vitamin deficiency, malabsorption, chronic renal insufficiency or failure.
Step 2: Baseline Lab studies:
CBC, reticulocyte count, iron panel
Step 3: Ensure adequate iron stores:
Iron saturation <30%:
____ Iron Sucrose 100 mg IV once a day x________________(total maximum dose 1000 mg or 10 doses )
Or
____ Iron Sucrose 300 mg IV every other day for three (3) doses
Step 4: Oral medications:
Folic Acid 1 mg PO QD
Vitamin C 500 mg PO QD
Vitamin B12 1000 mcg IM x 1 dose
Step 5: Epogen:
____ 20,000 units SQ three (3) times a week until hemoglobin >/= 10 gm/dl
____ Bloodless patient hemoglobin <5>/= 10 gm/dl
Step 6: Monitor and evaluate:
____ CBC, reticulocyte count 7 days from initiation of treatment